This is a post by Robert Watson. Robert is a retired Professor.
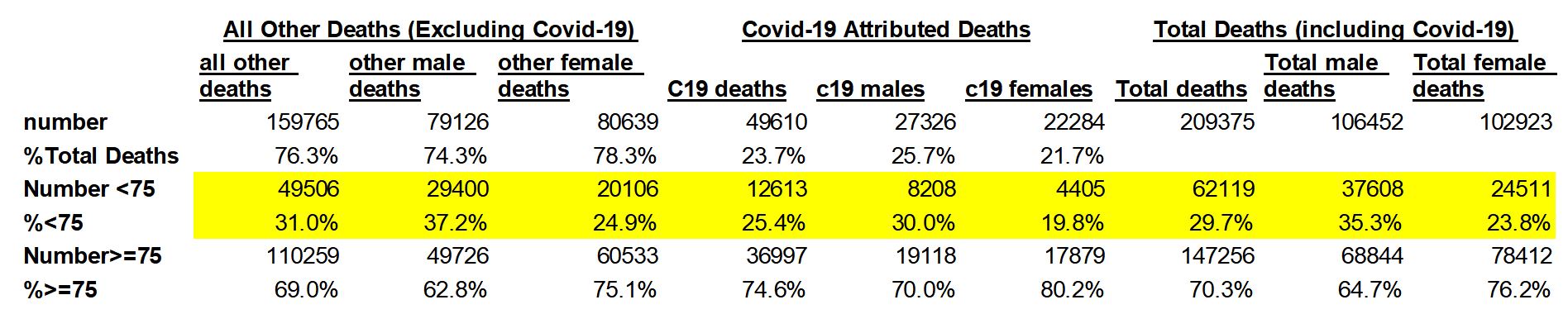
This post analyses the ONS mortality statistics for the first 25 weeks of 2020 taking account of the demographic changes and longer-term mortality trends of the population of England & Wales. Essentially, as Covid-19 appears to be a new disease – the first recorded death in England & Wales being in week 10, 2020 – the analysis separates out Covid-19 attributed deaths from all other causes of mortality. Thus, total mortality = all other causes + Covid-19 deaths. Despite the extraordinary public policy response to the appearance of Covid-19, it appears to be a fairly benign disease insofar as, to date, its primary victim group have been the very old and already terminally ill individuals, i.e., those already largely living on borrowed time. The summary table below provides an overview of the most pertinent issues addressed. (All images can be clicked to enlarge.)
Analysis of the Covid-19 ONS (attributed) mortality statistics indicate that the probability of otherwise healthy individuals (even members of the weaker sex, males) under the age of 75 or so dying from the disease is pretty low in both absolute terms and relative to all other forms of everyday causes of early mortality. However, by looking at the age distribution of the population and the long-term decline in premature mortality, it becomes self-evident that the potential size of the Covid-19-and-all-other-causes-of-death victim group has increased significantly over the recent past. This factor is, I contend, the primary explanatory variable driving the size and distribution of Covid-19 deaths in England & Wales since the first attributed death in week 10 of this year.
Premature Mortality (Deaths of persons<75 Years Old) and Demographic Implications
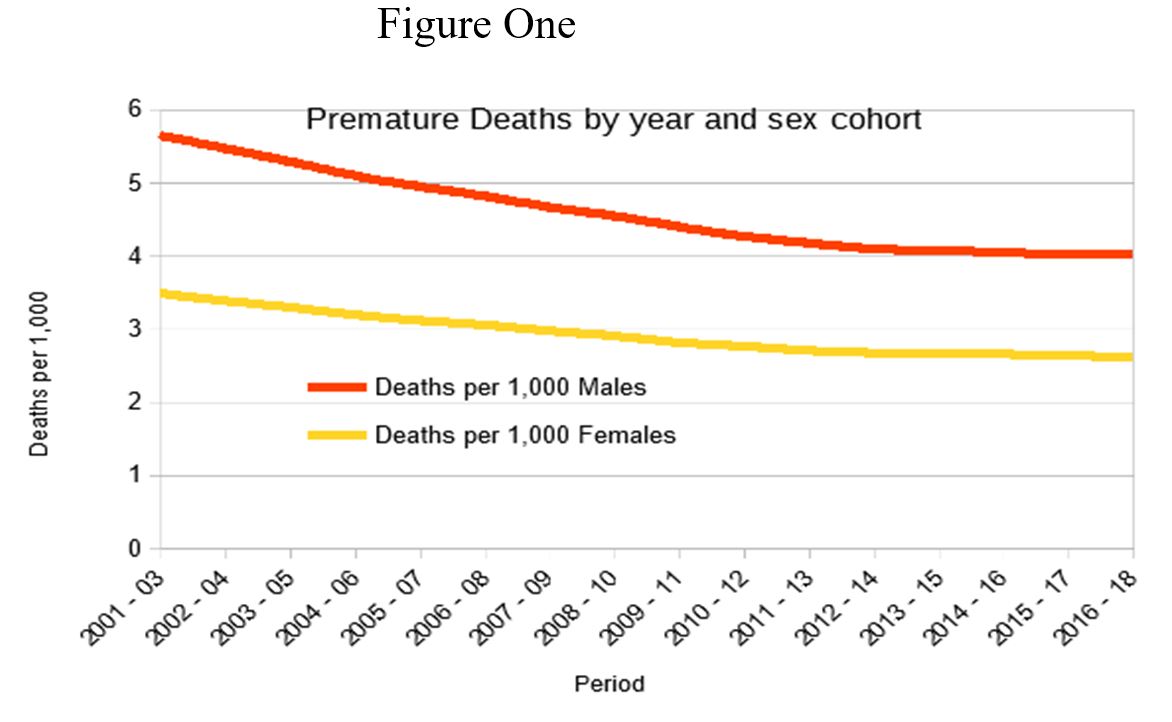
The notion of ‘premature’ mortality has been taken from Public Health England. Table One below presents the 3-year averages for the years 2001-03 to 2016-18 trends in ‘premature’ deaths per 1,000 of the English population, that is, the death rates of persons (and the split for males and females) below the age of 75. In addition, I have used the ONS 2019 statistics for England & Wales to calculate the premature mortality rate for 2019 which appear to be insignificantly different from PHE’s figures for the earlier periods. This suggests that the Welsh are unlikely to have been dying-off prematurely at a dissimilar rate to their English neighbours. Thus, their absence from the PHE figures seems likely to be immaterial in terms of the overall picture and conclusions be be drawn from the analysis. Figure One below provides a visualisation of the trends in premature mortality since 2001-03 to 2016-18.
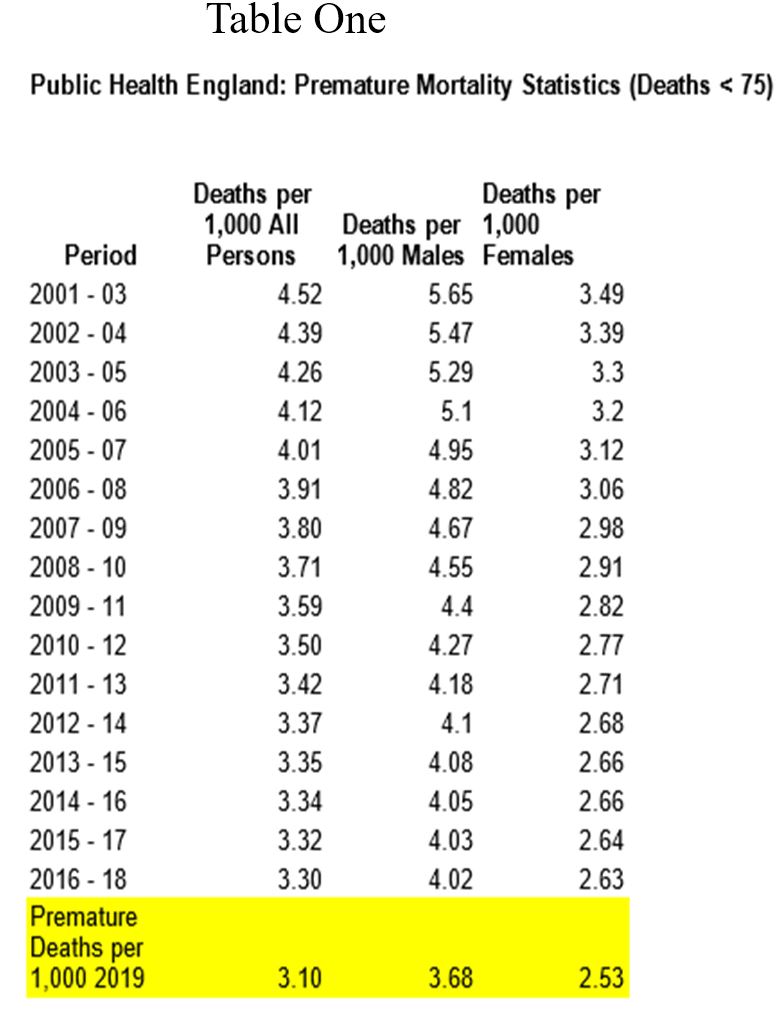
Though the age cut-off of <75 is to some degree arbitrary, as will be shown later, it is potentially very useful in that unsurprisingly the vast majority of deaths from all causes (including Covid-19) occur in the 75-and-over population. It also reminds us that though death is inescapable, we can take comfort from the fact that relatively few deaths are premature and that for the past twenty years the premature mortality rates (particularly for males) has consistently declined. In addition, the causes of premature mortality are generally well understood and, according to PHE, are to some extent preventable via the continuation of existing macro economic/occupational developments, more effective medical interventions, and individual behavioural changes.
As David Hume famously observed, there are no unmixed blessings in this world, and this is most certainly true in relation to the steady reduction in premature mortality rates. As the human race has not yet discovered the secret of immortality, the obvious corollary of the fall in premature mortality rates is that the population of old and vulnerable persons in the population increases; death is postponed not avoided. The costs of this postponement of an otherwise early death typically involves the acquisition of one or more painful and debilitating medical morbidities, the requirement to be institutionalised (euphemistically referred as being placed in an ‘old folks’ or care home), and the implied loss of agency and dignity in one’s declining years. As has become all-too-apparent over the past few weeks, any concentration of elderly people with severely compromised immune systems constitutes a huge risk factor whenever infectious diseases such as seasonal flu viruses and of course Covid-19 becomes rife in the (partially asymptomatic) wider population.
So, apart from the figures of lower premature deaths presented above, what other evidence is there to suggest that there has been a recently enlarged cohort of elderly people in England & Wales particularly at risk of dying of an infectious disease such as Covid-19? Table Two below presents the ONS population estimates (expressed in 1,000s, though the numbers in the spreadsheet actually go to three decimal places, i.e., down to the individual level) relating to England & Wales for 2018, 2019 and 2020 by age and sex cohorts. These 2020 population estimates I use later to standardise this year’s deaths to obtain the relevant deaths per 1,000 measures.
I have also added summary statistics (raw numbers and percentages) relating to the changes in population sub-groups (i.e., Male/Female and the under-75/over-than-or-equal-to-75 age cohort splits by sex) over the two-year period from 2018 to 2020. A graphical depiction of the 2020 Male/Female age-cohort size differences is also presented in Figure Two as this gives a strong visual indication as to why the PHE definition of premature death is far from wholly arbitrary. Note, the relative size of the individual age/sex cohorts is actually the net result of birth rates over the five-year span pertaining of each cohort, subsequent net migration and deaths. However, the almost precipitous decline in cohort size after the 70-74 hiatus (which represents the surviving, home-based, early post-war baby boomers of the 1945-1950 period), is dominated by deaths. Old people tend to die off in great numbers after the age of 75 (who could have guessed?), such that only around 14,000 individuals (11,482 of whom are female) are estimated to attain the age of 100.
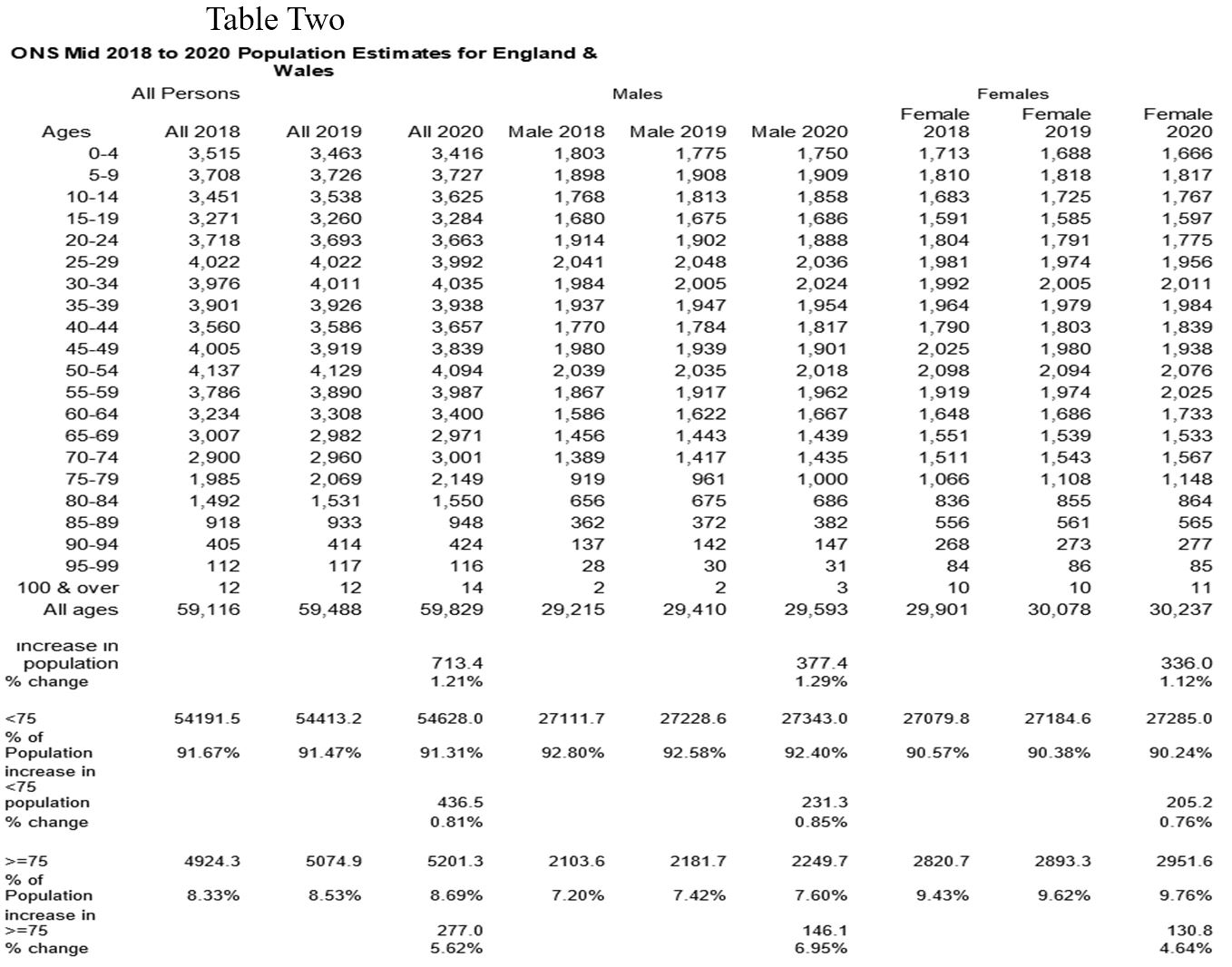

From the table, it can been seen that the overall change in the size of the population is estimated to have increased by 1.2% (713.4 thousand people) over the two years from 2018 – the respective male and female growth rates are 1.29% (377.4) and 1.12% (336). The under-75 age group is expected to have increased by 0.81% (436.5 thousand), whilst the >=75 age group is expected to have increased by 5.62% (277). The respective increases for males and females are 6.95% (146.1 thousand) and 4.64% (130.8). These figures appear to confirm the main implications of the declining premature death rates presented earlier; first, the elderly constitute an increasing percentage of the population, and that this increase in both numbers and percentages is most apparent in the case of elderly males; second, the over 75s naturally account for the vast majority of deaths and, of course, elderly males naturally tend to die-off earlier than their female contemporaries. Thus, the prime potential victim group (the >=75 age cohort) apropos Covid-19 has indeed increased by some 277 thousand over the past two years and now stands at some 5.2 million, whilst the more vulnerable of the two sexes, males, though around 670 thousand fewer than their female counterparts in total, has nevertheless increased proportionately more and now stands at circa 2.25 million.
Analysis of the ONS England & Wales Mortality Statistics 2020, Weeks 1 to 25
The summary table below (Table Three) indicates that by the end of week 25 (19th June), there had been a total of 326,627 deaths from all causes (Total Deaths). Relative to the prior five-year average of 272,626, this implies that there had been some 54,365 excess deaths since the start of the year. However, the first ten weeks of 2020 (i.e., prior to the first Covid-19 death) had been characterised by some 4,708 fewer deaths than the five-year average. In stark contrast, weeks 11 to 24 indicate there had been a total of 209,375 deaths from all causes and that this was some 59,073 excess deaths relative to the prior five-year average. As the total Covid-19 attributed deaths over this fifteen-week period only amounted to 49,610 this implies that there must have been 9,463 excess deaths not attributed to Covid-19.
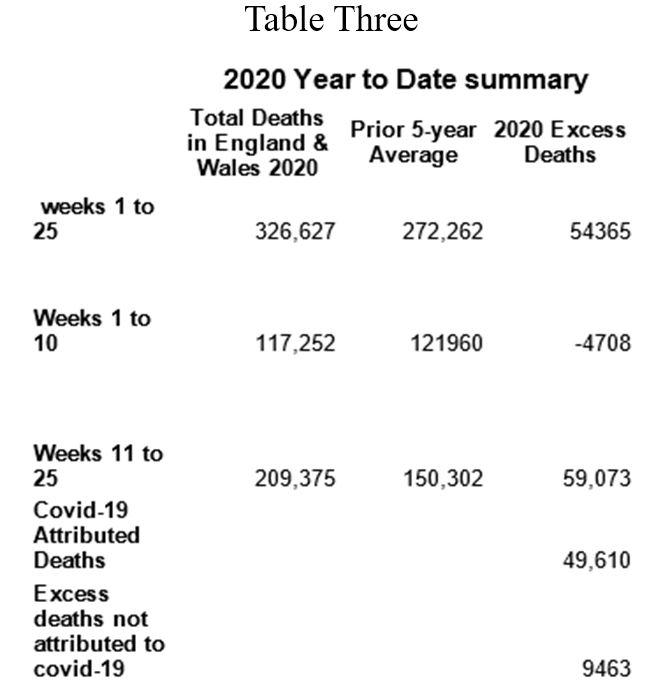
Given the fact that the NHS effectively closed down during this period in order to concentrate resources on the much anticipated tsunami of Covid-19 cases (and, as it turned out, for a significant proportion of NHS personnel to busy themselves with TikTok buffoonery) many of these excess deaths will probably have been due to patients being denied and/or being dissuaded from seeking medical treatment. Any claims to the contrary, such as these being ‘really’ unattributed Covid-19 deaths, run up against the obvious objection as to why we should bother having an extremely expensive medical system if its effective closure for three months doesn’t result in materially poorer medical outcomes for the populous!
The graph (Figure Three) below provides a visual representation of the year-to-date weekly pattern of mortality.
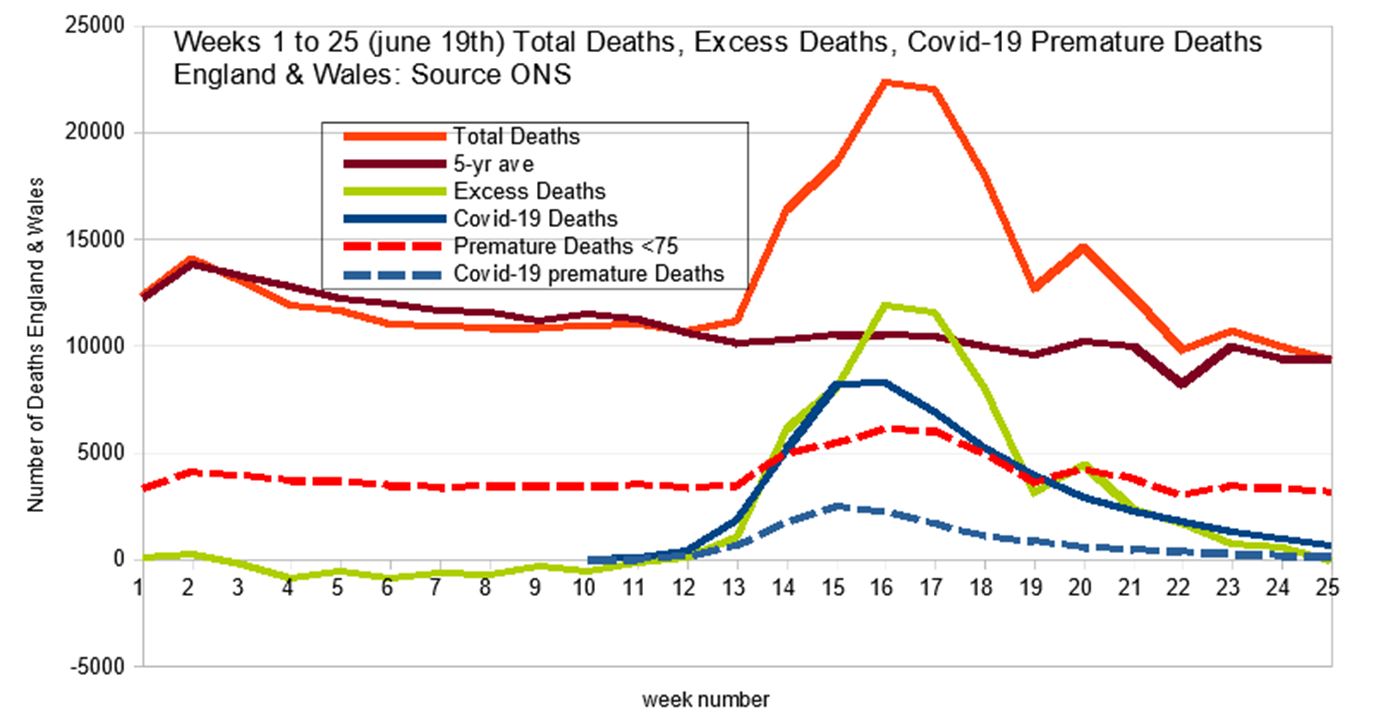
The Covid-19 and the excess deaths spikes track each other fairly closely and really began to take-off from week 14 (27 March to 3 April), some three to ten days after the commencement of the lock-down. However, the graph isn’t able to tell us whether the two spikes impact on the same demographic and/or whether there has been any material change over the subsequent fifteen weeks of the first reported Covid-19 death (so-called) pandemic.
The graph also shows the number of ‘premature’ deaths, that is, the number of deaths of persons below the age of 75 (PHE). PHE’s definition of premature death appears to have been particularly well judged as relatively few deaths are premature (approximately 29% of total deaths and 25% of Covid-19 deaths are premature), the main causes of which are predictable and fairly stable and, as the declining premature death rates over time suggests, becoming somewhat more preventable due a combination of societal and medical improvements and individual behavioural changes. In stark contrast, of course, the risk of dying (irrespective of Covid-19) necessarily increases exponentially after the age of 75 such that within twenty-five years of attaining this milestone survival probabilities all approach zero.
The graph (Figure Four) below presents the number of weekly male/female Covid-19 deaths and premature deaths.
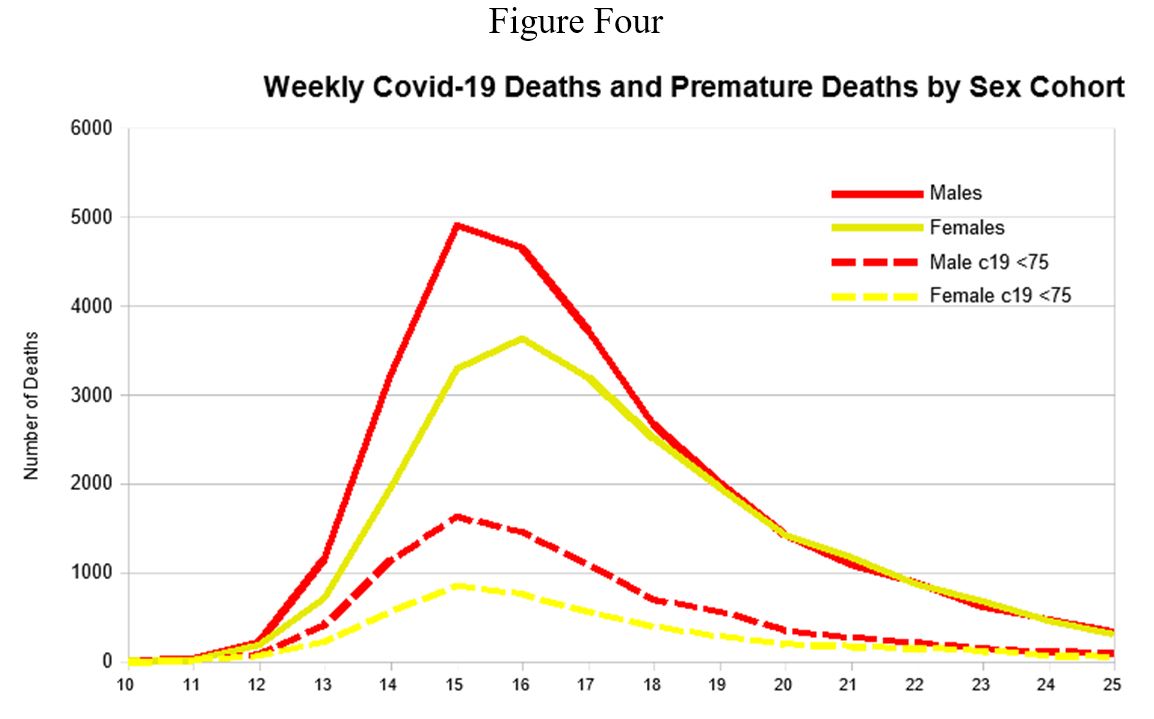
Of the total of 49,610 Covid-19 attributed deaths, some 27,326 were males and 22,284 females. For males, the Covid-19 spike peaked back in week 15 with 4,926 deaths. For females, the week of peak deaths occurred one week later with 3,621 deaths. Indeed, right from the start, up to week 20, male deaths attributed to Covid-19 were significantly higher than female deaths attributed to Covid-19. Since week 20 however the number of weekly deaths were to-all-intents-and-purposes evenly spread between males and females.
The total number of premature deaths from Covid-19 amounted to 12,613 and of these 8,208 were male and 4,405 female. These need to be compared with the much higher number of premature deaths from all other causes, 49,406 (males = 29,400; females = 20,106), over the same 15 week period. Both male and female covid-19 premature deaths also peaked in week 15 with a total of 2,511 premature deaths, 1,662 male and 846 female. So, male premature deaths attributed to Covid-19 over the fifteen-week period were almost twice as high as for females – in fact there was no week where premature female deaths were higher than for males – a result consistent with the significantly higher premature male death rate observed in relation to all other causes of mortality indicated by the PHE long-term premature statistics presented earlier. It should, however, be noted that Covid-19 is associated with proportionately fewer premature deaths for both sexes than all other causes of premature mortality, e.g., only approximately 25% of Covid-19 deaths occurred in people below the age of 75, whilst for all other causes of death 31% of those deaths are below the age of 75.
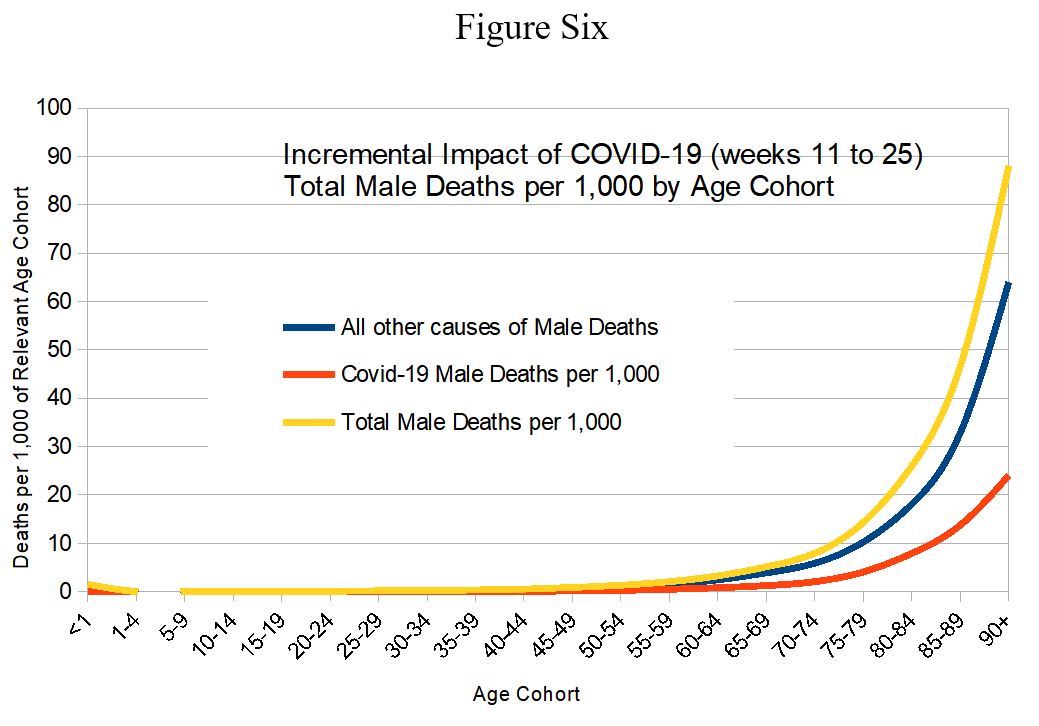
Figure Five below plots the standardised age and sex cohort Covid-19-attributed deaths, that is in terms of deaths per 1,000 as this metric controls for the differing sizes of the relevant cohorts.

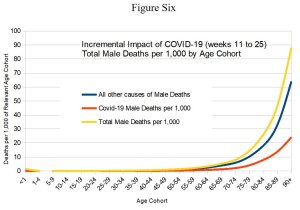
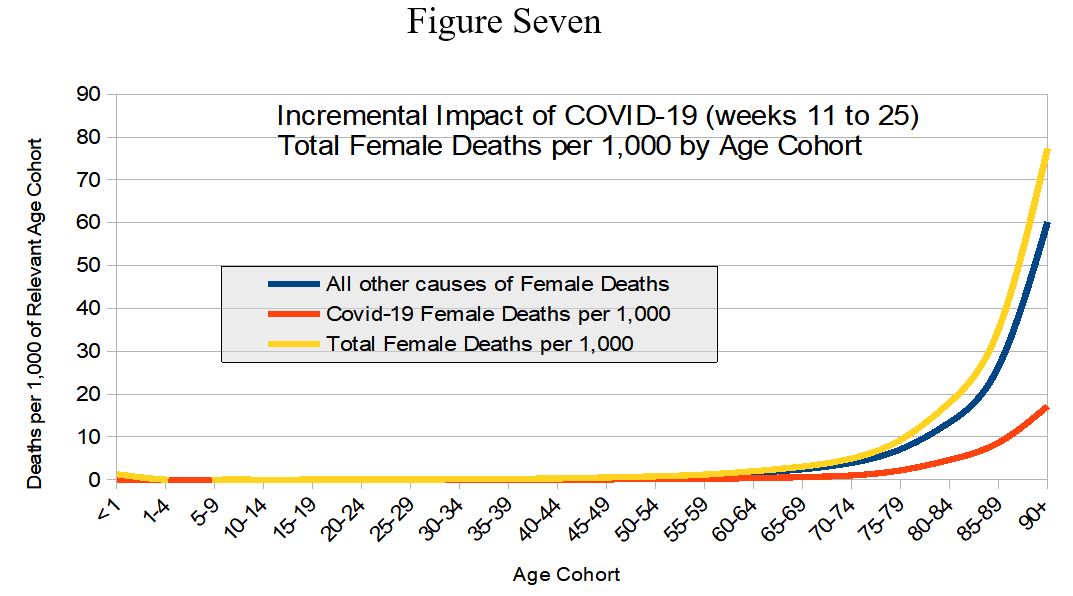
This graph indicates the extremely low mortality rates for persons below the age of 75 and how steeply mortality rates increase for both sexes upon reaching the age of 75. It also shows that at all ages male death rates exceed those of females by a significant margin. What the above graph does not show is the incremental impact of Covid-19 mortality relative to all other causes of death. This information can be gleaned from the two graphs below. Figures Six and Seven show the incremental impact of Covid-19 on respectively male and female total mortality rates for all age cohorts. Again, both graphs show that Covid-19 has a marginal incremental impact on mortality prior to age 75 and that the overwhelming majority of the deaths occur in the older age cohorts. Moreover, even for the most elderly age cohorts Covid-19 makes only a marginal, incremental contribution to overall deaths from all other causes, i.e., deaths from all other causes are between three and four times as large as that played by Covid-19.
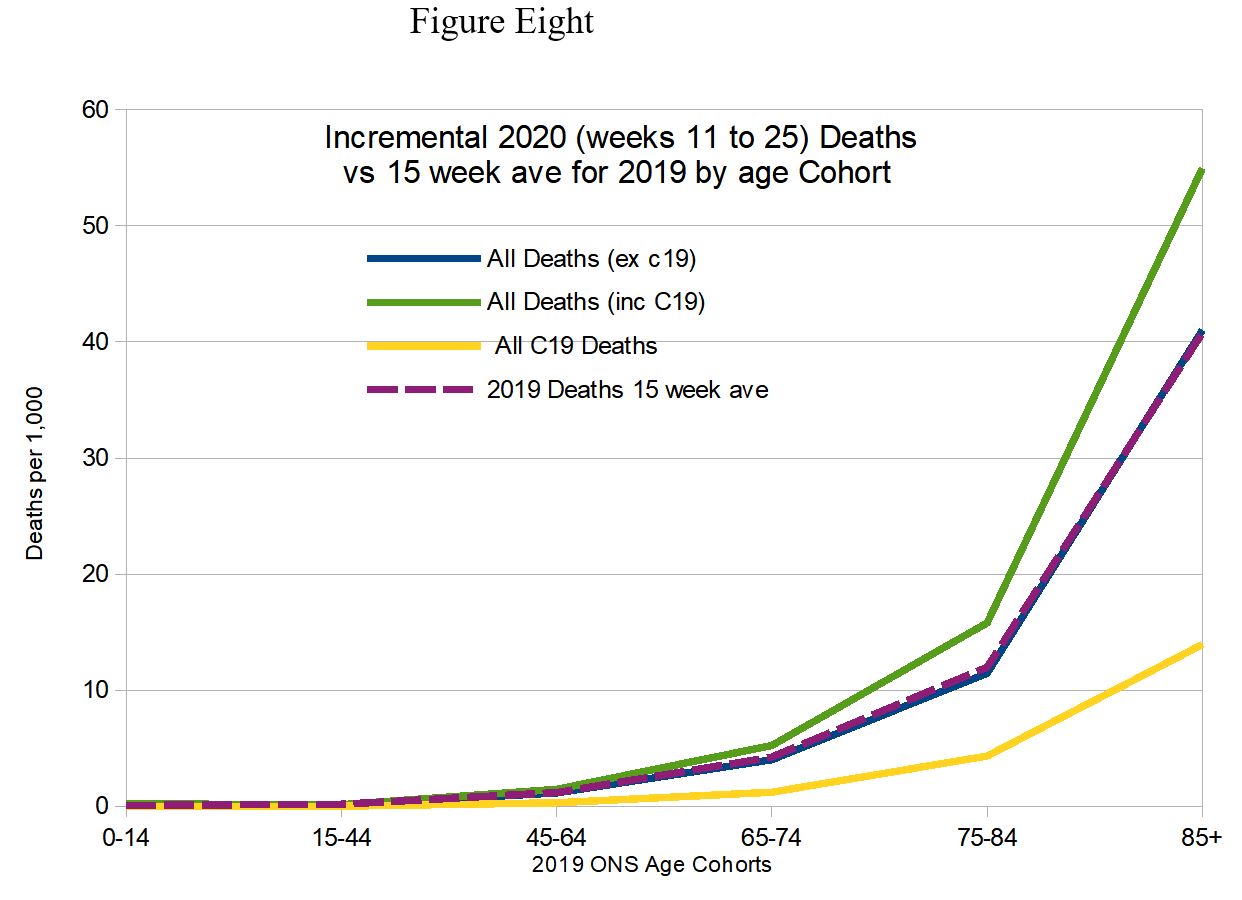
Finally, the figure below (Figure Eight) plots the incremental impact of Covid-19 using the 2019 ONS age categories and the 2019 15 week average total mortality profile, which provides the benchmark for the calculation of ‘Excess deaths’. As can be seen from the graph there are virtually no excess deaths below the age of 75, i.e., the difference (at the 75-84 marker) between the purple dashed line and the blue all-other-causes line, or even the total mortality green line. [Hector adds: the purple dashed line and the blue line are hard to distinguish because they mostly overlap each other.]
What this graph also confirms is that, despite the choice of time period – the fifteen weeks of this so-called medical emergency with its big scary spike that was going to overwhelm the health care system, etc. – some 75% of all Covid-19-attributed deaths have been amongst the over 75’s. In fact, rather than killing off the young and healthy (which would most certainly be a genuine medical emergency), Covid-19 simply reinforces normal and natural mortality patterns, only more so because as mentioned previously, Covid-19 is associated with a significantly lower percentage of premature deaths, 25% versus 31% for all other causes of premature mortality.
Concluding comments
The mortality statistics indicate that fearing death from Covid-19 for otherwise healthy people below, say, State pension age is essentially an irrational fear; i.e., definitely not based on any notion of science that I’m familiar with, but rather a neurosis lacking any firm empirical foundation.
To be clear, I am not suggesting that the public are incorrigibly stupid or incapable of making rational judgements. My interpretation of the evidence is that this Covid-19 neurosis has been largely induced by some relentless and shamelessly self-interested fear-mongering by the media, some shroud-waving members of the medical profession and other politically-motivated so-called academics. In short, the public appear to have been deliberately and systematically misinformed by their soi-disant ‘betters’. As a consequence, we have been saddled with absurdly and disproportionately destructive public policies. For example, inter alia, the closing down of large sections of the economy, non-Covid-19 medical services, large parts of the education system and the forced social isolation and distress caused to the already old and vulnerable.
The lock-down strategy, effectively ending the freedom of movement, association and assembly of the general population seems, prima facie, to be wholly disproportionate and counterproductive even from the excessively narrow mortality-minimising perspective typically adopted by the aforementioned miscreants disingenuously claiming to be guided by ‘The Science’. Well, there is no scientific justification for the mass incarceration of the non-elderly and relatively healthy population, i.e., those least likely to become even mildly ill from contracting (or even being aware that they have) the disease. Similarly, the mortality statistics fail to support the expectation that this will result in significantly increasing the longevity of the already very old and least healthy members of our society, the majority of whom probably would have died of something else within months anyway.
Whilst it is highly unlikely that this was their intention, it is nevertheless arguable that the seemingly idiotic reactions of public policy-makers to Covid-19 have brought about a state of affairs that more-or-less guarantees the fomenting of intergenerational conflict. Depressingly, the closest historical parallel is of course Mao Zedong’s Cultural Revolution, which (not incidentally) also resulted in an awful lot of older people (about one million) being violently dispatched by young Red Guards simply because the latter had been induced to believe that such people represented counter-revolutionary impediments to the achievement of unrealistic, State-sanctioned, utopian conceits.
Hector adds: We should all be very grateful to Robert for this article, he has put a lot of work into it, and it’s one of the best analyses of Covid-19 that I have seen. Sorry there has been a lull of a few days, I have been busy with various things, not least socialising on the weekend, but also continuing to act as an unpaid school teacher for my children, and helping out as an unpaid volunteer with another worthy project. As a result I have a bit of backlog of articles to go up this week, so if you’re waiting for yours, it’s coming. Please donate to keep the site going. Some people are doing this and I am very grateful to them. Following some requests you can now donate directly to me by making a Paypal payment, rather than going through Patreon or Ko-Fi. (I’ll put up a Paypal button as well sometime soon.)
20 thoughts on “Robert Watson: England & Wales 2020 Mortality Statistics in Context”
Very grateful to Prof. Watson for his very interesting and comprehensive analysis.
He has outlined and confirmed that which many of us have believed virtually from the start of this most ludicrous and embarrassing period in our history.
I remain both angry and frustrated at the manner in which this so-called pandemic has been mishandled, and I’m extraordinarily pessimistic about what might happen next.
Although, rightly, we should have great concern for the financial and employment crisis that appears to be just over the horizon (the so-called mini-budget will be interesting), my thoughts turn more towards the next time the bloody awful media we have in this country report on another virus.
What will “Jolly Japes” Johnson and his not-so-merry men actually do next time?
1) Tell us all that this time, there’s nothing to worry about, carry on regardless chaps! or
2) Go into Panic and Hysteria mode again and shut the country and its population down a second time? (and, according to whatever bug we get sent, the third time? the forth time?)
My feeling is 2) will never happen, simply because of the financial aspect. Surely, there’s no way any government could repeat this ridiculous exercise, now that they’re aware of the potential cost?
But, if the government become terrified of possible public reaction to 1) and panic, what then? And how the media, led by the BBC, might react is anyone’s guess, but I think what needs to happen is that the government should introduce legislation to bar the media from reporting ANYTHING in a sensationalist, duplicitous or mendacious manner. Judged by the manner in which these fools have disported themselves so far, this ain’t gonna happen.
As the old but very appropriate Chinese curse is supposed to have said, “May you live in interesting times….”
The collapse of the economies of the western world caused by the Banking system and the political elites post 2008 was inevitable and about to happen, Italy was poised to be the first domino to topple.
This virus came along at a perfect time so now it can be blamed for the crisis we now face and the perpetrators will be able to carry on, and now with their increasing powers, coincidence?, i think not.
@Christopher Stocks
Exactly.
As for the irrational fear of this virus, it was indeed deliberately induced by the government:
https://www.ukcolumn.org/article/covid-coercion-boris-johnsons-psychological-attack-uk-public
Others have speculated (I have no evidence of this) that the virus is being used as a sort of Trojan horse to usher in the U.N.’s Agenda 21 and Agenda 2030. See this utterly vile piece of globalist crowing:
https://www.weforum.org/great-reset/
Dark times ahead, economically if not socially. My contempt for Alexander “Boris” Johnson is now ineradicable and complete.
Many thanks to Prof Watson.
It’s not just the UK authorities, though. Virtually every government in the world has gone into the same state of unglued panic, which means that some other factor is at work?
Could it be the hyper-connectivity of the online world in general, and of ‘social’ media in particular?
Interesting that Prof Watson draws a parallel with the Cultural Revolution. It has crossed my mind frequently of late.
Since the introduction of mandatory muzzle wearing on public transport, which is leaching out into wider acceptance, starting with the new guidelines for the newly-liberated businesses, it’s clear to see that there is a huge psyop taking place. This morning I noticed the MSM are starting to push the public to demand muzzle-wearing. Just as with lockdown, the populace will clamour for the instruments of its own demise.
Prof Watson’s analysis clearly proves what has been evident for weeks now – that CV19 affects only the elderly and the ill and is pretty benign for the rest of the population. The lockdown was clearly unnecessary and has had disastrous social and economic effects.
So, the question is: Why is lockdown being prolonged? That’s where the focus needs to lie. From the responses here, some people are aware of which direction to look and the potential answers are more terrifying that any trumped-up pandemic.
An excellent take on this manufactured ‘crisis’.
Like others here, I am angry at the manipulation, and dismayed at the complicity that I see. The fall-out is inexcusable by any civilised standards.
Although I do see some signs of reality dawning, and a consequent slight increase in informed scepticism about the controlled narrative, many fellow citizens (or should I say ‘subjects’) are still insanely fearful. This is despite the fact that this was *not* a year of spectacularly high mortality when placed in a historical context, and even the higher than average levels of mortality can be partly attributed to an older and more vulnerable cohort of the population surviving the low infectivity of the previous year.
Beyond that, of course, is the fact that we have no way of properly knowing (beyond inference) the role of this virus, given the confusion with mortality effects of locking up society at large, and the lack of accurate source data.
I estimate that currently (using NHS England figures), that you will have to have a random 3000 people breathe into your face in order to come across one incidence of infection. And yet, we have today, the president of the Royal Society stating his opinion (based on some pretty dodgy ‘research’) that the wearing of face masks should be compulsory. In an astounding corruption of logical thinking, probabilities, risk assessment, and the basic medical principle of harm v. benefit, he compares this to the wearing of seat belts. I think the phrase is ‘Beam Me Up, Scottie’.
I have always been warily resistant to conspiracy explanations, but current life in the UK has become so distorted in so many aspects that I am forced to consider intentionality as well as cock-up in any explanation of these corruptions of society as evidenced in the above, and the recent manufacture of a ‘lock-up’ situation in Leicester out of …. no substantive evidence.
One objection to the “it’s all a conspiracy” idea is that to begin with people, and governments, were absurdly insouciant about the “Chinese sniffle”. There was an absurd under-reaction to what might have turned out to be a very cruel disease.
Eventually, it’s true, people and politicians over-reacted, mainly by panicking into clumsy, ill-targeted behaviour. Although protecting people in care homes could only be imperfect, at least a decent stab could have been made at it.
“this Covid-19 neurosis has been largely induced by … [amongst others] … politically-motivated so-called academics”: oh dear – are you suggesting that Professor Wotsisname is no mere charlatan? I must say that I’ve never understood why people paid any attention to a chap with such a record of consistent failure.
In Australia the government seems to have been more successful (so far) by adopting the strategy of ignoring the advice of its own medical men.
I have to say that I saw no signs of ‘an absurd under-reaction’, given the sad historical record of epidemiological modelling as exemplified by Ferguson and ICL on each significant prior event. That’s the problem with crying ‘Wolf!’
The absurd over-reaction stands proud, however.
I haven’t looked for a month or so now, but for much if the epidemic the rates of death per cohort over 55 from Covid had a constant ratio to normal rates of death in that cohort. The correlation was remarkable (over 97%). I’m unsure what that means, but it cannot be coincidence. I also strongly suspect “excess” non-Covud deaths are far higher than the raw data suggests. Not all deaths recorded as Covid are Covid, – at least some, perhaps many – are actually “usual” deaths that would have happened anyway. That means excess deaths are perhaps much higher than currently claimed, probably because care homes had a second infection (according to PHE, unknown what) and lots of avoidable deaths were not avoided.
In reply to Tim Hammond :
The noted correlation is well-observed. In essence, there is nothing strange about this year’s mortality, except, perhaps the timing of the April spike. Otherwise, it’s much like any other year of higher than average infection, and Covid-19 will simply be one of the agents that affects the larger than usual vulnerable population.
I’d pick up again on the term ‘excess’ deaths, which supposes a ‘normality’ against which numbers can be gauged. In fact, it is just a deviation of a projection from reality.
There are, of course, past mean and median values – but mortality varies both systematically and stochastically over time. An ‘excess’ over a ‘norm’ is just a theoretical construct – and we know where the ICL theoretical constructs got us!
As to Care Homes – there is no evidence that I can see of a ‘second infection’, and the degree to which deaths might have been significantly avoided is a question mark, given the overall large vulnerable population. This isn’t to excuse the obvious errors made in returning individuals from hospitals to Care Homes – but it seems clear that the victims mostly had a limited lifespan, and in general were subject to a range of serious comorbidity.
Unfortunately, we’ll never know, since the process of accurate attribution of death was comprehensively destroyed.
“the process of accurate attribution of death was comprehensively destroyed”
For fat old men with several serious illnesses there is no Platonic accurate attribution of death possible. Doctors look at a form, wonder what to write, suck their pens, and write down something reasonable: reasonable, not “accurate” . It clearly can’t be remotely as simple as attributing death to a car crash, a stabbing, or a drowning, say. I learned this lesson from an epidemiologist friend years ago, long before the current plague. But you can find a doctor being frank about the problem currently, to wit the admirable (and sceptical) Dr Kendrick.
https://drmalcolmkendrick.org/2020/05/31/covid-deaths-how-accurate-are-the-statistics/
“I saw no signs of ‘an absurd under-reaction’”: then it’s likely you started paying attention a little late in the day.
American here, for context.
It was briefly touched on in the article but I see very few British pundits on any part of the ideological spectrum that view these deaths as a failure of their socialist health care system. My main takeaway form the Italian debacle, for instance, is that their socialist health care system is as good as all their public works – ie total crap.
You Britons are forced to fund a very expensive health care system (are yall even allowed to purchase private insurance or pay with cash?), whose duties most definitely include properly handling epidemics and pandemics, yet has in my view completely dropped the ball. So instead of protecting YOU during a crisis (the entire point of the involuntary system) you’ve been imprisoned and your livelihood stolen yet are still required to foot the bill. To add insult to literal injury you’re coerced into clapping and cheering your incompetent oppressors from your prison cells.
I don’t think America-as-striven-for will remain intact for long, and not to insult or depress the obviously sane ones who frequent this site, but it seems to me England is and has been irreparably lost for a while.
Robert,
Superb article and good conclusion. Comprehensive and very informative analysis – every MP and journalist should read this
Pretty much confirms what I’ve being saying since Feb/March: a nothing-burger
I will spread your article
Many thanks
PS I liked the brief touching on morality:
“…As the human race has not yet discovered the secret of immortality, the obvious corollary of the fall in premature mortality rates is that the population of old and vulnerable persons in the population increases; death is postponed not avoided. The costs of this postponement of an otherwise early death typically involves the acquisition of one or more painful and debilitating medical morbidities, the requirement to be institutionalised (euphemistically referred as being placed in an ‘old folks’ or care home), and the implied loss of agency and dignity in one’s declining years…”
For the last 5 years of my grand-mother’s life she repeatedly said “I hope I die tonight”
@John Wilkinson
Spot on
Destination msm already flying too:
– https://c2n.me/48iJjZt.jpg
@dearieme
I too saw no signs of an absurd under-reaction.
On the contrary, I saw absurd over reaction from early March – when world mortality was ~0.5% of symptomatic. Hand-washing obsession and signs saying “Please pay by contactless card”
@Sam
Spot on. Private insurance – yes, but usually excludes A&E and infectious diseases.
eg https://www.bupa.co.uk/health/health-insurance
and https://www.axa.co.uk/private-health-insurance/
USA: If msm & Google et al succeed and Biden (AOC) wins sadly you are finished too and China becomes GloboCop
Pcar: For the last 5 years of my grand-mother’s life she repeatedly said “I hope I die tonight”
So many people nowadays tell similar stories about the unpleasant final years and lingering deaths of their parents or grandparents. Story usually ends with a statement like — I am not going to let that happen to me.
However, the Smith & Wesson solution to collapsing quality of life is tough — both on the departee and on those left behind.
There have probably been big changes in the experience of death in the Western world over the last half-century. It seems that the WWII generation saw their own parents get sick & die quite quickly — in contrast to the slow painful decline so many of them experienced themselves. In a rational world, politicians would be leading discussions about how to face up to the tragedy of lingering decline, because we all have a stake in that issue; every single one of us will face death eventually. And shunting the old off into “Care Homes” to linger & die deprives us all of dignity.
But we do not live in a rational world.
Brilliant by Professor Watson. Also good comment by Sam.
I do also wonder if the elderly population of the UK nudged further upwards in Feb/Mar 2020 as people returned from Spain among others to blighty, or didn’t leave on the first place because the cruises were being cancelled. It would be hard to tease out data for this, but I cannot it imagine the trend ( something like stopping 600k people a week who normally enter/leave the UK, or so I’ve read ) running in the direction of youth
Please could Prof Watson update this excellent analysis as I suspect the data will provide further evidence of how correct he was and how reactions by governments are even stupider.
@Pcar: “I saw absurd over reaction from early March”. Early March was late in the day. By early March even the dreadful WHO had noticed.
Early January was the time to notice – reports were in the papers but pooh-poohed. Hell, by Jan 12th China had handed over the genetic sequence.
Comments are closed.