
Here’s a very important and timely article from Thomas Galen. Thomas took a degree in Medical Sciences and then spent thirty years working with models and numbers in finance and with large businesses.
In the last few weeks those who claimed that the reduction in Covid infections in March was caused by herd immunity have been forced into retreat by the Second Wavers. This is a shame, as the Herders have a much better case, and the Wavers a much weaker case, than both assume. At the moment I see no reason to jettison the claim that Covid declined in Spring because of widespread herd immunity, nor the claim that we need to do very little now in the face of rising infections.
So what is herd immunity? Put simply it is the means by which people without immunity to a disease are prevented from getting infected with it. For a virus to spread, it must encounter a new person it can infect. Herd immunity denies it the chance to do so by having insufficient people who can be infected in its path. If a virus cannot find a new host before it is destroyed by the immune system of its existing host (or that host dies), then it vanishes. In most cases, herd immunity doesn’t require every person in a herd to be incapable of being infected (“immune”). You simply require a sufficient number of people with immunity because an infected person will not encounter every possible person (unless the herd is very small) before the virus is killed by his or her immune system. In practice you need to ensure that on average each infected person infects fewer than one other person. That ensures that an infection cannot spread amongst the herd, even if one or two members becomes infected.
The number of immune people required depends on the ease with which a virus is transmitted – the easier it is to catch, the more immune people you need. It also depends on other factors such as the size of the herd, patterns of socialisation and the composition of the herd (e.g. age, health, previous infection history). However the crucial point about herd immunity is that it doesn’t require 100% of people to be immune: in all cases it requires substantially less than 100%. That means that even if other forms of immunity are not present, you do not need everybody to become infected with a new disease to stop it spreading to everybody.
Which people are immune is a complicated question, partly because we don’t really understand our immune system very well and partly because we have very little knowledge of all the viruses that circulate. In general however there are four types of immunity: those with an innate immunity probably due to their genes, those who have previously been infected, those who have been infected with a similar virus that provides cross-immunity and those that have been vaccinated. One of the key arguments about Covid is what proportion of people fall into each of these four buckets and therefore how close to herd immunity or otherwise we might be.
In this context it is important to understand why herd immunity matters, even if we have a vaccine to a disease. Not everybody can be vaccinated – some are allergic, some have compromised immune systems – and for some vaccines are ineffective – for example, elderly people who have who have ageing immune systems. But herd immunity means that those people that cannot be vaccinated are protected from infection even though they themselves have no immunity.
Wavers claim that the current rise in infections is obvious proof that Herders were wrong. But this is based on a number of misconceptions about herd immunity. First, herd immunity does not mean that nobody ever again gets infected. Individuals can still do so but the infection does not then spread. Second, it does not mean that there cannot be new outbreaks of a disease. Herd immunity is not fixed in stone. It is naturally limited in time as people with immunity die and people without immunity are born. Without either a small churn of infection or vaccination, herd immunity will eventually disappear from a population, allowing a full blown epidemic. Third it doesn’t mean that people continue to benefit no matter where they are. Herd immunity only works for as long as an individual stays in that herd. It does not provide protection if you go on holiday to a place without herd immunity. Thus, if we see new Covid infections now, that does not prove herd immunity did not exist in March. What it could mean is that some herds have changed. Indeed, the nature of the new infections suggest that it did exist in March, because they would not appear in this way in a genuine, uncontrolled epidemic.
Why this is so is simple to describe. The important word is herd. A herd is a limited, local group. For most of us, we have what can be thought of as multiple herds. It is only when the herd immunity threshold (“HIT”) in all of these is reached that the members of the herd are fully protected. For example, if three out of four people in our homes have been infected or have cross-immunity, it will be impossible for the fourth person to be infected there. But if only five people out of twenty are immune at your work and only ten out of a hundred on the Tube then if you do not have immunity yourself you are not protected from infection because those settings have not reached HIT. This may explain why seroprevalence is higher in London than elsewhere: HIT is naturally higher in a large, highly mobile city with lots of comings and goings than, say, a small village in Norfolk.
Once HIT is reached in all the relevant herds, somebody without immunity is protected from infection. If the infection is introduced into that herd, it is very unlikely to spread. But that holds true only for so long as the composition of those herds does not change. Herd immunity is conditional on the percentage of people with immunity staying at or over HIT.
The obvious example is measles. For many years after the vaccination was introduced measles was rare – but importantly not non-existent. Each year there were a few cases but they remained both limited in number and localised, because vaccination amongst children and previous infections amongst adults provided herd immunity. That changed with the advent of the anti-vaxxers. In the past few years, particularly in the US, we have seen a number of outbreaks with over a thousand children infected across the country. That these are concentrated in areas with lower rates of vaccination such as New York clearly demonstrates the point. Previously, in a typical school of 1,000, around 950 children would have been vaccinated against measles. The remaining 50 were protected by herd immunity. But when vaccination rates fall below that level, to say 90%, herd immunity is lost and it is then possible for the 100 unvaccinated children to catch the disease. Note that it takes very little change to mean a relatively large number are at risk. A change of only 5% in the number vaccinated is sufficient to produce a large outbreak. [HD: ie. ‘large’ by modern standards.]
We see another example every year in universities. The annual ritual of Fresher’s Flu is real and probably caused by a virus or viruses. That it is caused by students lacking herd immunity is frequently alluded to even if it is not spelt out. The clue is on the name: it affects students in their first few weeks at university but rarely thereafter. It is also rare amongst second and third years. (Incidentally that suggests that at least on a university by university basis the virus is the same each year, which raises a number of interesting questions).
When a few thousand young people come together for the first time in September, they form a new herd often with little or no pre-existing immunity to the virus. After a few weeks, a sufficient number have been infected to reach HIT and the infection rapidly disappears. This is herd immunity in action every year, with a virus or viruses that must be endemic.
Some people describe such events as ‘seasonality’. That is just an observation however, and one that is not terribly helpful. Biology responds to stimuli, not calendars and decades of research has found little or no correlation with anything properly seasonal: temperature, humidity, rainfall, sunlight. Fresher’s Flu arrives on the dot a week or so after freshers arrive no matter what the weather. An Indian summer or an early frost make no difference. We see a similar effect in school children with a steep increase in colds in September.
What these events do correlate with are significant population movements. It is easy to underestimate the large scale of such movements in the UK each September and October. Around 2.8 million students go to university, including over half a million first years. Most go away from home, living and studying in close proximity to thousands of new people. At the same time, half a million graduates start a new job, often in a different city to their home or university. 1 million children start primary school for the first time, another 1 million start secondary school. 6,500 medical students begin their clinical studies in hospitals and a similar number start jobs as junior doctors across the health service. Those 6,500 new doctors cause a cascade of changes across the NHS. The data on other job changes is less available, but many people with children choose to change jobs and cities or districts in September to coincide with the new school year.
In addition, this year the government lifted restrictions on new residents in care homes at the end of July. Given the time required to organise a place it is a reasonable assumption that new residents started to arrive only in mid to late August. Infections started to rise steeply in care home at the beginning of September. The point about these new residents is not that they are bringing in the infection. That is not the issue and so testing and quarantining for fourteen days will not make a difference. The problem is that new residents who do not have immunity will disrupt any pre-existing herd immunity. That this happens in an environment where infections spread easily and with people who may be highly susceptible to infection is a problem. Let’s say we had a care home in July with 100 residents of whom 60 are immune and 40 are not. For this population, HIT is 60% and so infections have stopped. But if we introduce 10 new residents, all without immunity, then the overall percentage with immunity drops below the HIT, to 55% (60/110). That exposes the 50 residents without immunity to the possibility of infection. HIT is not reached until there are six new infections (and note that HIT can overshoot in any given herd).
A similar effect can be produced without new residents. If residents with immunity are hospitalised or die from other causes, the percentage left in the care home with immunity will go below HIT. This point is worth noting: care homes have a much higher rate of deaths and hospitalisations than the general population and those getting infected with Covid have a much higher rate of death too. That makes both reaching and maintaining HIT very difficult, as a significant proportion of those who would otherwise provide the immune population – people who have already been infected – are taken out of care homes. A significant proportion also suffer from immunosenescence, which may destroy previous cross-immunities. This makes care homes exceptionally vulnerable to all infections.
Outside of care homes, the population movements mean that around three million young people are creating new herds at schools, universities and in the workforce in September and early October. That’s 4.4% of the total population and (excluding the youngest) around 25% of the 10-25 population. If we add in other population movements such as changes of jobs and in care homes, it is quite possible that 6% or more of the UK population is on the move, changing the composition of existing herds and creating new herds. This has knock-on effects outside the new herds with spillover to local communities via pubs, clubs, restaurants and other facilities and contacts – a university sports team of perhaps fifty people having an initiation ceremony in a local pub creates a huge new risk of infection for the locals who had happily reached HIT over the summer.
It is no surprise therefore that autumn usually sees a significant rise in respiratory diseases and a concomitant rise in deaths. There is a redistribution of people and consequently a redistribution of immunity. It is the redistribution that matters, not the total number of people who are immune.
If Covid is following this pattern rather than a Second Wave, what we would we expect to see?
First, a rapid rise in infections amongst students and young people. Second, an uneven distribution of infections across age groups, correlating with what proportion of each group moves at this time of year. Third, a lack of infections in areas where there are fewer population movements and where any such movements are less disruptive of pre-existing herds – typically areas with smaller towns, more rural areas, and fewer big universities that attract widespread admissions. We would also expect to see infections in care homes increasing sharply rather than in a typical infection pattern, and renewed problems with hospital infections, both of staff and patients. This is the pattern we see, quite clearly.
There’s also something we would expect not to see: a widespread epidemic amongst all age groups and across the UK as a whole, with a classic infection growth rate. We now have a much smaller number of people without immunity than in March (assuming 20% or so have now been infected) and not every herd is new or has been disrupted. Thus the infection is now spreading amongst the much smaller number of people with no immunity, and the number of infections required to re-establish HIT is, in most cases, quite small.
We can illustrate this with some data. Since 1st September, 91 NHS trusts in England (41%) have not recorded a single Covid death. The percentage recording 2 or fewer is 54%. Now these are not trusts that at the height of the epidemic were recording very large numbers, but for comparison the 54% of trusts with 2 or fewer deaths recorded 13% of hospital deaths back in the Spring versus only 2% now. At the other end of the scale, a mere 19 trusts (9%) are responsible for 50% of total hospital deaths since 1st September. In Spring, those Trusts accounted for only 21% of total deaths.
We can also look at the speed of the epidemic in spring versus now. The graph below shows cumulative deaths over the two periods: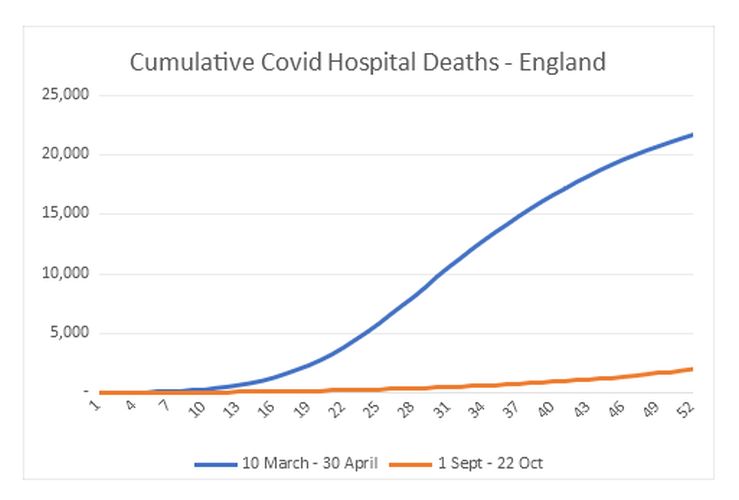
What this shows is that in two periods each of 51 days, the rate of increase in deaths is completely different. So far, there is simply no sign of a widespread, fast-moving epidemic. For those under 60, the difference is even more stark: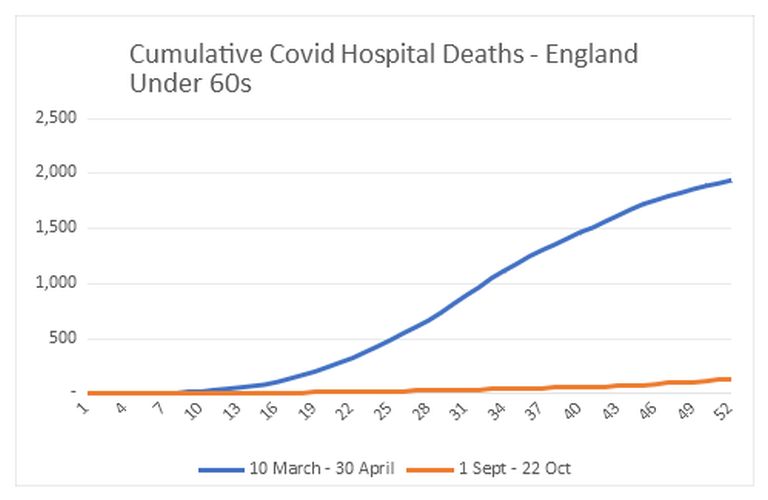
This sort of growth is not at all characteristic of an easily transmitted virus in which the vast majority of people are susceptible. It looks far more like a virus that is currently difficult – but not impossible – to transmit.
None of this means things won’t change and we won’t see a genuine widespread revisitation of the Spring epidemic. But to date infections and deaths conform to the Herder hypothesis, not the Waver.
We can look at that hypothesis in a bit more detail. A Second Wave relies on two key assumptions in Imperial’s model: that up to 90% of people can become infected because Covid is a new virus and second that lockdown and other measures prevented the vast majority of the population from becoming infected.
At this point we cannot claim that the evidence against that is incontrovertible, but it is considerable. The fundamental problem is that infections clearly peaked before lockdown and their decline did not accelerate when lockdown was introduced. Indeed, it is difficult to see the effect of any of the numerous interventions or contraventions of the regulations (e.g. demonstrations) on the infection curve. Its shape follows almost exactly what a modelled infection without effective interventions would look like. There is also significant evidence that there is a ceiling on the proportion of people that can get infected, and that suggests it is considerably below Imperial’s estimate. In numerous cases of closed environments – cruise ships, aircraft carriers, care homes, homeless shelters – we see time after time that at most 30% of people get infected. We simply do not see very high levels of infections (we might possibly in some Indian slums but those numbers come with significant caveats). A virus that could infect up to 90% of people and which kills 10-20% of the frail elderly when infected ought to have devastated care homes. There were far too many deaths, but nowhere did we see anything like that. Instead a proportion got infected and a significant proportion of those died, but in no care homes did we see 80-90% of residents testing positive. Even if most care homes were able to somehow stop infections in their tracks, there should have been at least two or three that failed to do so. But there were none. And if not there, then where?
It is however unlikely that HIT is 20-30% for Covid, so if we cannot find anywhere with much higher rates of infection then how do we square the circle? It requires a significant proportion of people to have some form of cross-immunity. There is increasing evidence for this, not just the observational data from closed environments but also laboratory data too, suggesting that there is widespread T-cell immunity from previous coronavirus infections. That in turn ties in with data suggesting that a large proportion of people who are infected do not develop antibodies to Covid but instead fight it off with T cells alone. That in turn fits with the hypothesis that the elderly who are most vulnerable to Covid may suffer from immunosenescence which largely affects recent T-cell immunity.
The fact of cross-immunity is well-established. The first vaccine, for smallpox, was derived from cowpox, a closely related, but not identical, virus. Indeed, evolving an immune system that gave us as wide cross-immunity as possible would be clearly hugely advantageous, so it should be no surprise if that has happened. We know there are a number of coronaviruses that cause colds as well as those that cause more serious diseases such as SARS and MERS. It is likely there are others that we have not yet identified – it would be interesting to see if graduates were less likely to suffer from Covid than non-graduates as a result of Fresher’s Flu, for example. Cross-immunity might explain why previous widespread epidemics of coronaviruses such as SARS and MERS did not happen.
Allowing for both direct T-cell immunity and antibody prevalence in the UK suggests that perhaps 20% of the population has been infected, not the fewer than 10% that the UK government claims. Back-calculating the total number of infections using deaths and a reasonable IFR gives a similar figure: 45,000 deaths and an IFR of 0.3% suggests 22% of the population infected. If a further 40% of the population already possessed cross-immunity, then we had sufficient numbers to have reached herd immunity in March.
We can therefore cast serious doubt on the government’s claim that 90% of us can still be infected. Indeed, the government’s forecasts about a Second Wave could only happen if ALL of the following are true:
-
lockdown restricted the percentage of people infected to a very small fraction of the population, even though it was introduced after infections peaked;
-
the subsequent phased release of lockdown somehow resulted in no increase in infections because the government’s relaxations were perfectly judged;
-
all those who have been infected have antibodies to Covid;
-
there is no cross-immunity from other coronaviruses;
-
the IFR is 2-4 times higher than most current estimates.
To put it another way, despite Covid being a new virus, despite lockdowns and other measures being wholly untried and extremely blunt instruments, despite knowing few, if any, of the key metrics of the virus such as the IFR, Imperial’s model got everything exactly right. That would be an extraordinary achievement. The chances of it happening are essentially zero. No model ever gets that much right, every model needs adjustment from its initial assumptions as real-world data come in. But not Imperial’s, apparently.
Nor is the notion that the government got everything perfectly right until we started to misbehave remotely credible. For a start, it is logically inconsistent – was our misbehaviour not predicted correctly as part of the assessment? But even allowing for that, it would be miraculous for the various intricate restrictions that have been put in place, relaxed, put back, modified, relaxed and so on to have worked so perfectly. This should have been, inescapably, a matter of trial and error, with consequent ups and downs, not a series of brilliantly executed manoeuvres resulting in the smooth and constant reduction in infections after mid March. Frankly it is delusional for the government to think the latter.
If the herd immunity hypothesis is correct, we can make some general predictions. First, infections in universities and amongst young people should start to fall rapidly. That may have started already. There will be some spillover to non-students but that should be limited. Second, there will not be a general, widespread second wave across the country and across all age groups. Rates of infection will stay unevenly distributed across age groups. Third, deaths will increase only slowly and stay relatively low. Fourth, Covid infections will quickly retreat and not reappear until there are other substantial population movements.
We could even do a back-of-the-envelope calculation about infections and deaths. If we assume that (i) 7 million people have changed herds (the movements outlined above plus the people affected indirectly), (ii) 10% of that number have already been infected and (iii) we require 20% of people to have been infected to reach HIT (with a further large percentage having cross-immunity), then we would expect to see 630,000 new infections. So far, since 1st September we have seen around 350,000 new infections. We probably haven’t found all the infections though. If we have found two-thirds, that means there have been 530,000 in total. Allowing another twenty days to reach the total would mean an average of 5,000 a day. That seems possible but requires the infection rate to start to decline soon. It’s a very rough estimate but we can see quite quickly at least the trends hold true.
Where does all this leave us? The arguments revolve around a handful of numbers – what percentage of the population can be infected, what percentage of the population already has some immunity, what percentage of those infected will die? For all the moral grandstanding of recent weeks, the argument comes down to those figures: 90% or 30%? 0% or 40%? 1% or 0.3%? These are things reasonable people should be able to disagree on without calling each other names. Believing we may have substantial cross-immunity cannot possibly make us evil, any more than believing that we don’t have cross-immunity can make somebody stupid. A sensible government would recognise this and accept that neither side has a monopoly on truth, let alone on ‘the science’. Unfortunately, we have a government that has determinedly taken a side when there is neither the need nor the evidence to do so. Instead we have reignited the panic and alarm when it is still not clear if that is appropriate or necessary.
Update: Please support this website by donating via KoFi, subscribing via SubscribeStar or Patreon, or buying my book (see right-hand sidebar for links). Independent media like Hector Drummond Magazine, and my constantly updated Twitter account, cannot survive without your support.
19 thoughts on “Thomas Galen: What Herd Immunity Looks Like”
Para 14, final sentence. Why is the number without immunity 30? I would expect it to be 40+10, rather than 40-10.
A Care Home ‘herd’ needs to include all employees who are not resident and who are likely to be the source of any new infection now that discharge of infected elderly patients from hospitals has been stopped.
The carers will all come from their own community herds and often work at several different homes. To obtain Home herd protection from a low percentage of immune residents, the number of external challenges must be strictly limited or the definition of what constitutes the Home Herd needs to be greatly extended.
ADH, I’ve changed it to 50, thanks.
Further thought. The percentage of the population with immunity that is required to provide herd immunity will vary according to people’s interactions. If everyone behaved like a hermit (the perfect lockdown) it would be zero. If everyone kissed a hundred strangers every day it would be best 100%.
Also if lockdown was imposed after infections reached their peak it would have no effect and neither would a return to normal. This seems largely to have happened in London.
If the lockdown is applied before infections have reached their peak they do have an effect, which ends as the lockdown ends. This appears to be happening outside London, indicating incidentally that the lockdown did slow the course of the disease at least a little.
Basically in as much as lockdowns work, that work is undone as soon as they end.
So we either extend the current charade for ever or we accept that unpleasant diseases have unpleasant consequences and deal with it.
Very good article.
As the virus appears to cause no symptoms in many or most people, then surely this will greatly restrict the spread and aid herd immunity. Is that being factored in or isn’t it relevant?
Very interesting article but there are places with infection rates as high as 60% as 2 studies of Manuas show.
“The important word is herd.”
Correct — that is the important word. That is the word which shows our Betters want all of us to think of ourselves as dumb stock animals who have no idea where to go until our Betters hit us with an electric cattle prod.
Let’s get off our knees! Orwell was right — control of the language gives the Political Class control of our thoughts.
They call the current outbreak of another of the many “Influenza Like Illnesses” which are observed every year a “pandemic”, even though the UK ONS looked at the data and noted that Covid-19 in September was only the 19th (19th!) most common cause of death in England — and even lower in Wales. Some “pandemic”!
They call healthy people who happen to test positive for the presence of some RNA (in a testing regime which the inventor has said is inappropriate for this purpose) “cases” — even though those people are not genuine medical cases (i.e. sick people).
And while our Betters spread fear with their Lock Downs (aka electric cattle prods), they ignore their own economic insanity in printing money and killing businesses while China’s industry roars ahead producing the real goods & services on which we in the West increasingly depend. Let there be no misunderstanding — we will pay a heavy price for destroying our productive capacity and turning the West into a Cargo Cult economy.
We have to acknowledge that common sense & reality have lost the argument on the CovidScam, but at least we can stand up and use the appropriate words. We are talking about Population Immunity — groups of human beings, not herds of dumb animals.
All very good stuff, but completely undermined by the uncritical acceptance of “cases” – and even “deaths”.
The number of “cases” relies on the PCR test, whose inventor categorically warned that it was not suitable as a diagnostic test. It also produces a significant number of false positives, but that too is secondary. The PCR technique can amplify stray fragments of RNA and, as Mullis said in so many words, can be induced to detect anything you want it to.
https://uncoverdc.com/2020/04/07/was-the-covid-19-test-meant-to-detect-a-virus/
https://www.youtube.com/watch?v=FHx059IqP_M&feature=youtu.be
The alleged number of “Covid-19 deaths” is also meaningless, as no one can be sure whether a given death was due (wholly, mainly or partly) to Covid-19. People are going into hospital with all sorts of conditions and are automatically tested on admission. If they test positive and later die, they are often counted as “Covid-19 deaths”. Meanwhile, total deaths from all causes, are almost exactly the same as for previous years, proving that there can be no enormous number of deaths due to Covid-19.
Please note that, since January 2020, not only the UK but most countries worldwide have reported virtually no deaths from flu! https://www.iceagenow.info/flu-cure-discovered-video/
Which seems more likely to you: that flu has suddenly packed its bags and left the planet, or that deaths due to flu are now being counted as due to Covid-19?
Interesting analysis, testable prediction made and generally a good read, cheers Thomas for this article.
Covid-19 is going to become an endemic common cold virus.
It will take with it a sizeable percentage of end-of-lifers who get it, as common corona cold viruses do (https://www.hindawi.com/journals/cjidmm/2006/152612/), and will otherwise be a kiddies’ sniffle. The bulk of the middle of the population will be immune, or mostly only mildly ill if they get it.
Spread that paper – show the world that common or garden coronaviruses kill 8% of vulnerable people and for decades we just took it in our stride.
That is how to kill this madness.
Thomas, Excellent article, thank you. I will share
Which Prof do you believe?
Bias by omission or bias for funding (money)?
.
@Hugh R
Hancock announced several times over last few weeks: Covid positive patients will be discharged back to care homes to free up beds for surge. Care homes must isolate them
@BiG
Good to see you’re finally backing what I wrote in early March
Congratulations
Good article, needs sharing, a lot.
I see Tom Welch commented on something similar:
With regards to T-Cell immunity and not getting Covid:
The amount of immunity is likely way higher than what is being estimated as there still is the issue of attribution. From the source data used in Northern Ireland’s decision to lockdown, one paper showed flu and Covid cases. 20,000 people presented with possible Covid and they were tested. 96% of these were not also tested for flu.
The reason given was that the labs were overloaded with tests for Covid which had priority. So a resource issue then led to incomplete information. Added to this is that Covid has higher reporting priority to flu even though the symptom list is practically identical. Even the supposedly unique identifiers are found with colds, pneumonia and flu. No baseline was taken to compare rates to be able to make attributions. Doctors were using subjective evidence i.e. chest x-rays showing scarring, with no reference to times when the flu caused the same thing.
We can see this in the numbers for flu deaths. Explanations abound all above the threshold for Occam’s Razor. The reason flu deaths dropped is most likely because the Covid deaths would have been labelled flu in previous years.
So it seems Covid-19 appears to only affect a very small subset of people well below the standard operating threshold for society. If proper measurements had been taken then we wouldn’t be having a discussion about herd immunity. We wouldn’t have locked down.
How does “Covid killed the flu” fit with “more people have been dying of the flu than Covid since June”? I think the figure was ten times as many flu deaths.
@mhcp
Spot on
Attend hospital for x-ray & cast removal from healed broken arm, test positive
Three weeks later admitted with Flu, die. Covid death
Long read
https://lockdownsceptics.org/how-covid-deaths-are-over-counted/
@Matt H
Yep, iirc x5 from mid May then by end June x10 peaking at x12 mid/late Aug followed by miraculous sudden decline when PHE lumped all SRS deaths together
An enjoyable read.
I think the best hypothesis of why there was no previous widespread epidemic of coronaviruses such as SARS and MERS, is that these were very serious viruses (IFR of 10% and 35%) and individuals were only able to spread the virus once symptomatic, and a large percentage because symptomatic – which made isolation of cases and elimination possible.
@ Charlie
Conditions in Manaus were chaotic, so virus spread was far more rapid. In those circumstances, the overshoot on herd immunity level can be substantial. Also not sure that studies have really looked at the levels of natural immunity: as a relatively isolated population, Manaus could easily be “different”. Remember, the diseases brought by the Spaniards to Latin America wiped out large parts of the existing populations.
Comments are closed.