
An article by Daphne Havercroft. In 2015 Daphne retired from a career as a senior project and service delivery manager for a global IT services corporation. She has seen and experienced the very best of NHS care, delivered by skilled and caring health professionals, and also the worst of the NHS, particularly its leaders’ callous attitude towards the elderly, which has been exposed for all to see during Covid-19. Her Twitter account is @DaphneHavercro1, and her blog can be found here.
Earlier this year a study was conducted to establish the prevalence of frailty in patients with COVID-19 who were admitted to hospital, and to investigate the association of frailty with mortality and duration of hospital stay. The report was published on 30th June.
The researchers concluded that assessment of frailty is crucial to inform clinical decisions about COVID-19 treatment and urged its use as a key indicator to assess a patient’s risk of dying.
It is not surprising that frail patients are at higher risk of dying of Covid-19 and it follows that assessment of frailty is also likely to be crucial to assess a patient’s risk of dying of other potentially serious illness, such as ‘flu.
One of the researchers commented that if people believe that they fall into the high frailty category they should ask their GP for an assessment. This is a tall order when many GP practices have used the excuse of Covid-19 to close their surgery doors to patients and deny them face to face consultations.
GPs have never been employed by the NHS. They are contracted by the NHS to provide defined services. One of the services is to proactively identify patients with moderate to severe frailty. Covid-19 does not release GPs from that contractual obligation.
This is the latest published version of the GP contract.
Pages 33 and 34 are informative. The Contractor (GP) is required to take the following action, not wait for patients to prod them into action:
- Annually identify any registered patient aged over 65 living with moderate to severe frailty by using the Electronic Frailty Index (EFI) or equivalent.
After wading through online NHS documents I eventually found this NHS England list of indicators of frailty:
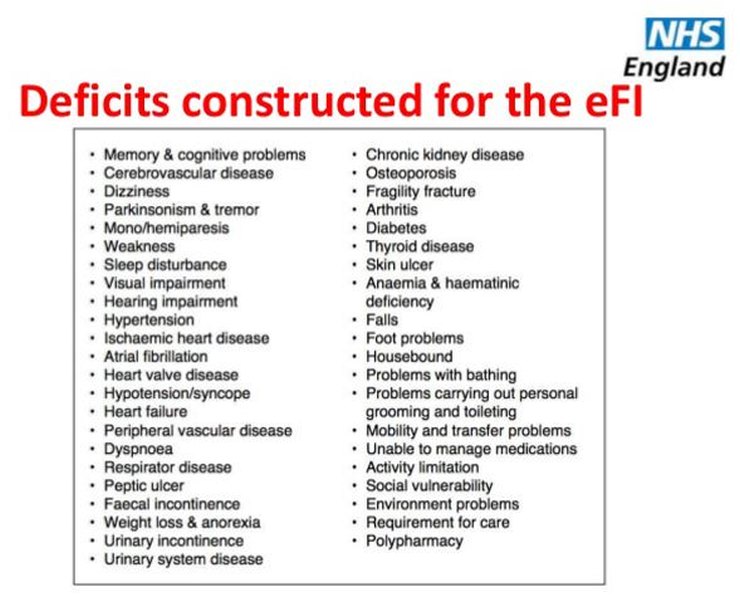
For patients assessed to be severely frail, the GP is contractually required to:
- Undertake a clinical review to include an annual medication review and history of any falls.
- Provide the patient with other clinically appropriate interventions; an example is physiotherapy.
- Instigate a discussion with the patient about an enriched summary care record, described here with two examples which record the patients’ wishes about resuscitation.
It has been alleged that NHS managers responded to Covid-19 by telling care homes to put blanket ‘do not resuscitate’ orders on all residents. Every care home resident should be registered with a GP. On admission to the care home every resident’s GP should have discussed and recorded their wishes about resuscitation as part of a documented care plan. The resident and their family should have been be fully consulted on the care plan. Therefore there should be no circumstances, not even a pandemic, where an NHS manager is allowed to impose a blanket ‘do not resuscitate’ policy on care home residents.
I have never met anyone aged 65 and over with obvious frailty who has been formally assessed by their GP. If this lack of compliance with the GP contract is widespread, and it seems to me that it is, it means that the NHS is not performance managing its contract with GPs, thereby allowing them to avoid providing the primary care services that they are paid public money to deliver. The risk this poses to patients is avoidable deterioration in health which makes them more susceptible to unplanned hospital admissions and poor outcomes, including death.
The Department of Health and Social Care has recently produced more Covid-19 propaganda:

Some people may think that they are protecting Grandma by wearing a face covering, not hugging her and clapping like a chimp for the NHS. Good luck with that.
I suggest that a much more effective way of protecting Grandma (and Grandpa too), is to help her to make sure that her GP provides her with the primary health care services that she is entitled to receive and which the taxpayer pays for.
If her family doesn’t have the courage to do that for her, they can be sure that the Covid-19 obsessed NHS won’t either.
Update: Please donate or subscribe to keep this website going – see links on the right-hand sidebar.
Update 2: Note that the NHS poster above is real. There has been some discussion on social media about whether it’s fake, but you can confirm it’s real by going to the ‘Uk government’ Facebook page.
9 thoughts on “Daphne Havercroft: Covid-19, frailty and the NHS contract with GPs”
Daphne, informative, thanks
Re Poster/Ad
+1 for Peter Hitchens:
Also
https://twitter.com/ClarkeMicah/status/1300461853483708416
Hi, talking to a medical professional yesterday. Their main concern was the high death rate of treatment personnel. So, just wondering, can anyone confirm. Is the medical profession, hugely disproportionately represented in the death numbers?
SM, all the reports I have seen on this say no.
https://healthcareleadernews.com/covid-19/nhs-staff-no-more-likely-to-die-from-coronavirus-ons-analysis-shows/
Though as care workers have a higher rate it appears prolonged close contact with an infected patient might increase risk. I work with doctors doing out of hours house calls. This is mainly as paid shifts on top of working elsewhere in the NHS. A few stopped doing house calls. Most continued.
The changes were that previously they all worked in normal clothes and used gloves for examinations. Post Covid most now do house calls wearing scrubs. The now wear full PPE – visor, disposable gown, gloves. They reduce contact time by taking the history by phone before going into the house. One referred to doctors who stopped seeing patients as like someone who joined the army but wanted out at the sound of gunfire.
As far as I am aware only one of the doctors I work with has tested positive. A healthy 59 year old he was unaware he was infected until tested under the track and trace programme. His contact was his receptionist who caught it at a funeral not at work.
In hindsight he thinks a symptom may have been his daily jog a touch harder than normal but really not much more than normal variation.
@SM
Hector is correct
@Iain C
Absurd behaviour. Are doctors as brainwashed as most people?
Or
Are they following orders from GMC, NHS, Health Commission?
Thanks for that. Tells me that the healthcare worker are and are expected to be at a higher risk of infection. Acknowledging that healthcare workers risk a slightly elevated risk of death from infection. Though given the risk predominantly appears to be to those healthcare workers already suffering preexisting condition, including age.
So, is it a fair conclusion to make, that younger, healthy (under 60’s, without conditions) healthcare workers have minimal or little risk of death from infection? That would be in line with the general population.
My next question, there appears to significant media attention given to the damage to vital organs (lungs, heart, etc), caused as a result of infection. Media focus, on experts, that suite the narrative. Is there any evidence that infection causes long term permanent damage, to those whom recover? Or, is this too early to determine?
There’s a lot of media hysteria about it, but very little in the way of hard facts. The Times ran a story early on about long-term effects, with one guy who was struggling to recover as their illustration. Then a few months later they ran a similar story, again with one guy who was struggling to recover as their illustration. It was the same guy. He didn’t have any organ damage, just finding it hard to get back to normal (which happens with flu too).
The early hysteria about ground glass opacities in lungs has mostly disappeared.
There’s bound to be a small number of people who suffer organ damage, this happens with flu as well, but anything more significant than a few cases has not been shown. As Covid has been killing people for six months there should be plenty of hard evidence for this by now.
>Their main concern was the high death rate of treatment personnel
I don’t get this. It’s like joining the Army and then running away when you hear the sound of gunfire.
24th August 2020 “PHE downgrades PPE requirements for GPs administering flu jabs”
http://www.pulsetoday.co.uk/clinical/phe-downgrades-ppe-requirements-for-gps-administering-flu-jabs/20041386.article
The whole article might be hidden behind a registration wall, but these are some of the main points:
“GPs do not need single-use PPE such as gloves and aprons when working in vaccination clinics, according to new guidance from Public Health England (PHE).”
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/910885/COVID-19_Infection_prevention_and_control_guidance_FINAL_PDF_20082020.pdf
“Dr Fay Wilson, the GP in charge of Birmingham out-of-hours provider Badger, told Pulse the new guidance is ‘just about saving money’.
She said: ‘Someone has just suddenly realised that if we’re going to vaccinate half of the population against flu, that means we’re going to have to have 30 million pairs of gloves.’
‘I’ve seen people with hand gel, quick squirt, quick rub and that’s it. It’s not the same as changing your gloves.
‘You might as well wear a clove of garlic around your neck.’
Maybe hanging garlic round your neck is a better bet than relying on GPs who hide from their patients!
Regardless of Covid-19 and adequate PPE, the NHS Long Term Plan is to reduce face to face consultation with GPs by way of “digitally-enabled primary and outpatient care”
https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf
I don’t have a problem with that in principle. Who wants to sit in a doctors’ waiting room in winter with people coughing and sneezing if it can be avoided?
Whether the Department of Health and Social Care and the NHS can be trusted to deliver any of this successfully, and most importantly, humanely, is another matter.
@SM
Healthcare workers – msm being London centric concentrated on peeps there where many are in the more vulnerable non-white cohort. They are much more likely to suffer from co-morbidities (not always diagnosed) inc asthma, diabetes, high blood pressure, obesity, sickle cell. On obesity: sit in a hospital and marvel at how many NHS staff of all colours are obese
Long recovery happens to some with all illnesses. Dr Ellie Cannon (DM & BBC) said numbers no diff from Flu, Cold etc. Again, it’s msm fear mongering
Latest: 10 times more dying with Flu than C-19 – where’s the Flu lockdowns etc?
@Daphne
Thank you
Comments are closed.