This is an article by Peter Forsythe, who lives in Hong Kong. This article was originally published on Peter’s blog here. For some lovely photos of Peter’s garden and the nature surrounding his place, go here.
If lockdowns were effective, you would expect a correlation between the stringency of the lockdown and the number of cases or deaths per million. For while correlation does not (necessarily) imply causation, the opposite is true: causation does mean correlation. Hence: the stronger the lockdown, the fewer the cases or deaths per million. That’s the theory.
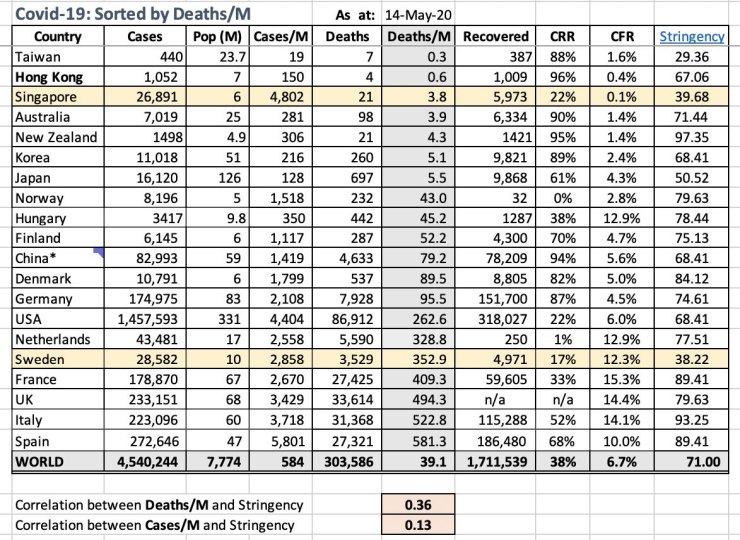
I did the figures, based on a ‘stringency index’ put out by Oxford University. 100 being the most stringent. And I did the correlation between this and the cases/deaths/ million, which come from Worldometer, run out of Johns Hopkins University.
The long and short: there is no correlation.
(Go here to view the spreadsheet.)
A figure of less than 0.6 means little or no correlation. Here the figures are 0.36 for correlation between stringency and deaths/M and 0.18 for same and infected cases/M.
So, there is – at least according to the figures we have so far – no correlation between the strength of the lockdown and the number of cases and deaths per million. This could change, and I’ll keep an eye on it.
By the way, the two countries with yellow shading are those with low levels of lockdown (according to Oxford University). I’ve just noticed that Taiwan ought to be shaded yellow as well (my bad). My own Hong Kong is at the middling-to-lower end of stringency, but world-best in terms of cases and deaths per million.
Singapore would likely have a higher ‘Stringency Index’ as it has implemented ‘circuit breaker’ measures since the Oxford figures, which are as at March 30.
It seems to be the case that high levels of cases and deaths/million led to severe lockdowns, rather than the severe lockdowns leading to lower levels of each. And note also that the top/best performers above, in terms of deaths per million (which the spreadsheet is sorted on), are all in Asia and Oceania. The top seven.
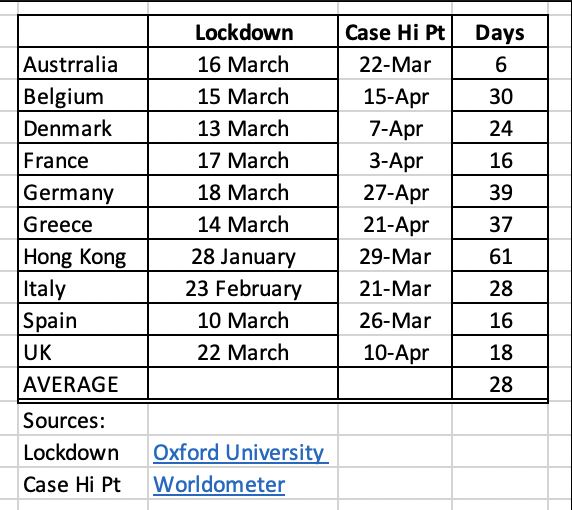
Update: This is my spreadsheet of the dates of lockdown, as defined (by me) as being the date that the Oxford U ‘stringency index’ for the country in question went above 50. And the date of peak infections, taken from Worldometer. I don’t want to make too much of this as there are many factors involved, such as the extent to which people did or did not follow the lockdown strictures, the measurement of the cases, etc. Still, it’s interesting that the dates vary so widely. You’d expect them to cluster around 14 days, the incubation period. But they vary from 6 to 61 with an average of 28 days between the lockdown and the peak of cases.
10 thoughts on “Peter Forsythe: Are Lockdowns Effective?”
Thank you very much for this, Peter! Those are vital numbers, which should have been basic input to all government policy making for weeks now (if not months).
Of course there may be some “softness” in some of the figures themselves. One feels that some governments may have done everything they could to “pad” the numbers, making the epidemic appear much worse than it really is and thus justifying their policies.
Have you seen Andrew Mather’s latest presentation at https://youtu.be/SheiRcaPAtM?
He does go through his slides very rapidly, but even without following all the mass of figures you will quickly get the drift. Statistically speaking, it is an open and shut case.
1. Infectious disease cases and deaths normally follow something like a bell-shaped curve. Rates go up, and after a while they go down. They never go “sideways” for days or weeks on end. Yet some of the graphs for Covid-19 do exactly that – notably the USA and my own country, the UK. Almost as if someone had orders to keep the fire burning until… when?
2. It would be reasonable for the peak of deaths to follow about 4-5 days to 2-3 weeks after the peak of cases. Yet in some countries the two peaks coincide, and in Denmark (from memory) the deaths peak came two days BEFORE the cases peak. As Mather says, people seem to have died before they become ill.
3. The very worst-hit countries (according to official figures) are the USA, UK, Belgium, Holland… right next to the US, UK and EU HQs. Poor countries have barely been touched (whatever their climates).
4. In the East, it looks like a different disease altogether. Some nations have zero percent infections, let alone deaths. Why?
5. The USA has by far the most cases (1,570,583) and deaths (93,533). That’s 283 deaths per million people. Second in number of cases is Russia (299,941) – but only 2,837 deaths! That’s 19 per million people. Odd.
Very interesting, although I would ignore Russian figures – I don’t think that they are trustworthy. Saying that I do agree with you
Funny you should say that, David – as it happens the figures I distrust are those for the USA, UK, and some other European states. I think they are probably inflated. (If you look at their graphs, you will see a LOT of “sideways” numbers – plateaux on the graphs).
I’m not sure about some of the numbers given here:
Incubation period – above says 14 days; https://www.acpjournals.org/doi/10.7326/M20-0504 says 5.1 days.
Dates of lockdown: above has Germany on 18 March, UK on 22 March; More or Less yesterday said both happened on 23 March (I also found different LD dates for Spain, Italy, France, Belgium… not sure which is correct but it seems to be “in the eye of the beholder” to some extent)
I don’t see Belgium in the list of “Stringency” vs D/M etc
Cases numbers are known to be highly variable – subject to all sorts of distorting factors. Deaths also but less, so might be a more reliable signal for “peaks” e.g. UK and Germany both LD’d on the same day (according to MoL) and both were around peak deaths over the same few days approx 15-17 days later.
No investigation of the point in the outbreak (eg number of deaths) at which LD was imposed. Might be an important factor in the eventual DpM etc.
On the more general point, it’s clear that (with the exceptions of Sweden and Japan) all countries listed had more or less the same level of LD but have very different DpM. This is then taken to be evidence for the irrelevance of the level LD in affecting DpM.
I don’t think this follows. As an analogy, in all countries in the world, murder is a serious offence, punishable by decades in jail or, in some cases, death. Yet murder rates vary from e.g. 2.6/M in Japan to 520/M in El Salvador. Much the same legal punishment yet a factor of 200 between them. Obviously other social, economic and cultural factors account for the differences. But I don’t think anyone would therefore conclude that having a law against murder doesn’t make any difference.
In the same way, widely varying DpM doesn’t imply that having/not having LD makes no difference. It sets a boundary within which other factors influence DpM
@Peter
Thanks, useful analysis
@Tom Welsh
Like you, I believe UK deaths inflated by Gov’t order to justify lockdown and by Left & MSM to attack Gov’t: Death recorded as CV if patient coughing, if self-quarantine falls down stairs, death recorded as CV, or in NI if they tested positive in last 28 days – if BoJo died tonight it would be CV death
Tory UK Gov’t shooting foot – again
German figures: probably accurate as Germans like accuracy
Orientals: they seem at less risk than whites and much less than non-white/yellow
Poor countries low deaths – malaria prophylaxis
Pcar,
Agree entirely about inflated numbers etc.
I’m interested in your last-“Poor countries low deaths-malaria prophylaxis”. Two weeks ago my GP, a sensible and pragmatic woman, gave me a prescription for a painful sinus headache, something I’v had on and off for years. The scip was for Doxycycline, an anti-biotic. Unusually for me, but “lockdown” boredom induced me into reading the leaflet, a version of which comes with all meds these days.
I read that Doxycycline is also an anti-malarial treatment and it appears one can take it on a fairly liberal basis as an effective medication for that condition.
Referring to Dr. Google, I then had that confirmed, but I also saw that Doxycycline is, following a very basic on-line “diagnosis”, freely available to purchase. I was under the impression that anti-biotics were strictly GP prescription only?
Some companies selling it did carry warnings stating that this drug does not treat CV19, which, being a virus and Doxycycline being an anti-biotic, I already knew. If Hydroxychloroquine can treat CV19 (open to debate, I know) and is also a well known and respected anti-malarial treatment that’s been around for many years, can anyone tell me if the two drugs are related in any way?
To be clear, I’m not hoping that my scrip can save me from the lurgy, (a pox on that) but merely wondering if there’s any connection. Childish I know, but the two names have similarities. Anyone like to comment?
Incidentally, I’m one that believes entirely in the idea that BigPharma ie. Gates, GSK, Roche etc will do anything to discourage the promotion of cheap, easily obtained treatments, in order they may sell their own extraordinarily costly snake-oil. I believe this is why existing drugs like Hydroxichloroquine are dismissed out of hand or scorned by these people.
@John
UK Gov’t banned export of Chloroquine back in February shortly after reports surfaced showing taking it prior to infection can prevent CV19 infection taking hold. They’ve never explained why. The denial now of efficy started as soon as Trump endorsed it
Doxycycline – don’t know, what are ingredients and chemical formula?
Why Dr prescribed:
https://bnf.nice.org.uk/drug/doxycycline.html#unlicensedUse
I rarely read leaflet as I don’t want to know side effects – too easy to self-induce
Similar name: Sodium Chloride and Sodium Chlorate !
Florida Governor Ron DeSantis lashes out at media over coverage of coronavirus
https://www.youtube.com/watch?v=Ebl3JWFruK0
Bangladeshi doctors find 93% success in CURING covid-19 with two cheap easily obtainable drugs; doxycycline and ivermectine. Even WHO is finding this difficult to refute or say they are dangerous drugs. Apparently previously Australian researchers had found ivermectine, a drug taken for worms, destroyed almost all the RNA of coronavirus.
https://zeenews.india.com/india/covid-19-cure-in-sight-bangladeshi-doctors-claim-ivermectin-with-doxycycline-can-treat-coronavirus-patients-2285317.html
Sorry was going to say re article, that Euro Momo WEEKLY excess deaths are now showing exactly what you would expect from a viral epidemic , bell curves. Almost everywhere is now at or below trend across Europe, having declined exactly the same way as increased. UK is still an anomoly, its pausing slightly in the decline.
Comments are closed.