
This is a guest post by Robert Watson. Robert is a retired Professor.
This post analyses the ONS England & Wales weekly data relating to ‘COVID-19’ and ‘All other causes’ of deaths (Total deaths – Covid-19-attributed deaths) for the weeks 11 to 16. The purpose of the analysis is to assess the relative deadliness of COVID-19 vis-a-vis all other causes of death and to evaluate whether the pattern of COVID-19 deaths in terms of age and sex cohorts differs significantly from the relative frequencies observed apropos ‘all other causes of death’.
Essentially, two main empirical questions are addressed. First, do COVID-19-attributed deaths appear to be a ‘new’ source of deaths that results in a large and possibly permanent increase in total deaths relative to existing death rates from all other causes? And second, to what extent does the pattern of COVID-19 deaths differ significantly from, or simply replicate, existing age and sex cohort fatality patterns?
Spoiler Alert
The analysis indicates that:
(i) whilst COVID-19 is most certainly a new cause of death, its victims are predominantly older men (75+) and very elderly women (80+); as both these cohorts are already very small (particularly so in the case of males) and also suffer from very high rates of death from all other causes, COVID-19 deaths only make up a small minority of the deaths (many of which would have occurred anyway within a few months); hence, it seems highly unlikely that COVID-19 will result in a long-term increase in death rates even amongst these vulnerable age cohorts.
(ii) Covid-19 does not kill off young people at all or even the middle aged to any significant extent; indeed, the pattern of deaths largely replicates existing patterns of deaths from all other causes; moreover, COVID-19 actually marginally reinforces the existing pattern of early male death rates
and the very high death rates experienced by the very elderly of both sexes;
(iii) as a new ‘killer’ disease, COVID-19 has the benign characteristic of choosing its victims from the already elderly, i.e., it is best seen as reinforcing the natural order of death; essentially, is there an alternative age cohort that one would rather this new disease decimates?; COVID-19 really would be a human life game-changer if it drew its victims from the young and/or otherwise healthy people in their prime of life!
(iv) If the blither being put about in the media that ‘every life saved is worth it’ really is to be taken seriously, then it is clear that we ought to forget about COVID-19 and instead throw vast medical resources at trying to reduce the existing massive premature slaughter of males in their 40s, 50s and 60s.
COVID-19: initial analysis of the ages and sex of its victims
The ONS does not currently have and/or publish information relating to the within-age and sex-cohort differences in pre-existing health status. In consequence, this analysis of relative COVID-19 mortality rates can only be based on the average for each sex and age category.
(Knowledge of the pre-existing health status of the COVID-19 fatalities relative to other members of their age and sex cohort would be beneficial in identifying, treating and advising those individuals most exposed to additional mortality risks.)
The time period, weeks 11 to 16 inclusive, was chosen due to week 11 (week ending March 13) being the week in which the first alleged COVID-19 death in England and Wales occurred, and week 16 (week ending April 17) being the week with the most recent figures to be published by the ONS (on the 28th April). The ONS provides weekly data relating to Total Deaths From All Causes and a separate COVID-19 Death count. In what follows, it has been assumed that both the Total Deaths From All Causes and the COVID-19 Deaths are correct. Even though, in relation to the latter, due to a lack of 100% testing for COVID-19 and the fact that a substantial majority of the alleged COVID-19 fatalities also suffered from other serious medical conditions at the time of death, it is less than certain that all of the COVID-19 assigned deaths were in fact due to COVID-19.* Nevertheless, all COVID-19 assigned deaths were deducted from the ONS total deaths from the all causes figure in order to obtain our benchmark comparison ‘deaths from all other causes’ numbers.
(*For instance, from the 28th April data release, ‘Because of the coronavirus (COVID-19) pandemic, our regular weekly deaths release now provides a separate breakdown of the numbers of deaths involving COVID-19. That is, where COVID-19 or suspected COVID-19 was mentioned anywhere on the death certificate, including in combination with other health conditions.’)
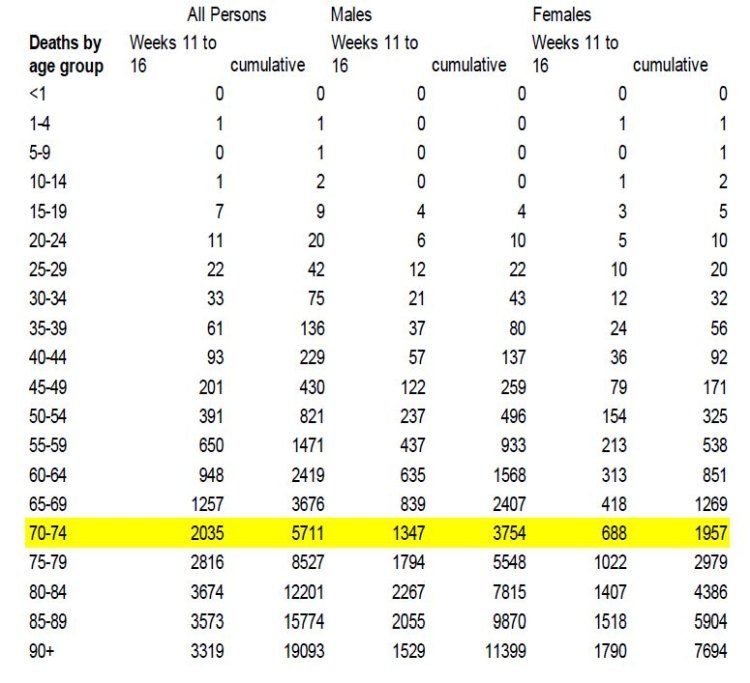
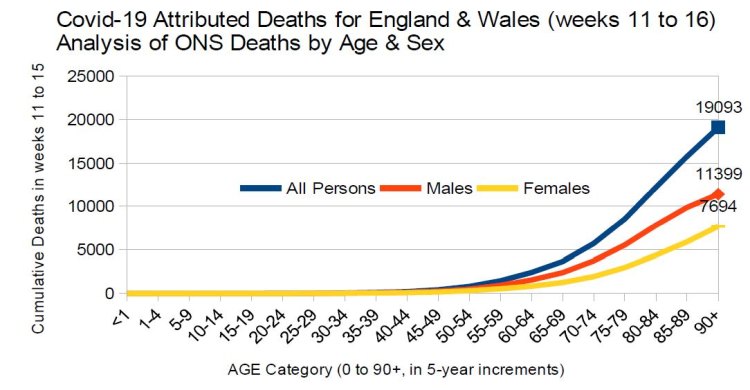
An initial analysis of the week 11 to 16 ONS death data indicates that COVID-19 deaths were largely restricted to older males (75+) and females (80+). See the table of figures and the chart below, which suggest that COVID-19 fatalities appear to broadly mirror existing death patterns, i.e., the large majority of deaths occur in the oldest age groups, and that COVID-19 tends to kill 50% more males than females and at a somewhat younger age. What this analysis is unable to establish, however, is the fatality rates in terms of deaths per 1,000 of each of the relevant age and sex cohorts. This turns out to be of some importance due to the relatively small size of these age and sex cohorts.
Comparative Deaths per 1,000 Analysis
In order to obtain a metric of deaths per 1,000 of the relevant age-sex cohort, which is required to make a valid comparison between the relative importance of all other causes of death and COVID-19 deaths, it has been necessary to obtain the estimated ONS projections for mid 2020 (published in October 2019) of the population distributions by age and sex of England & Wales. These are reproduced in the table below, along with a chart that provides a graphical representation of the data
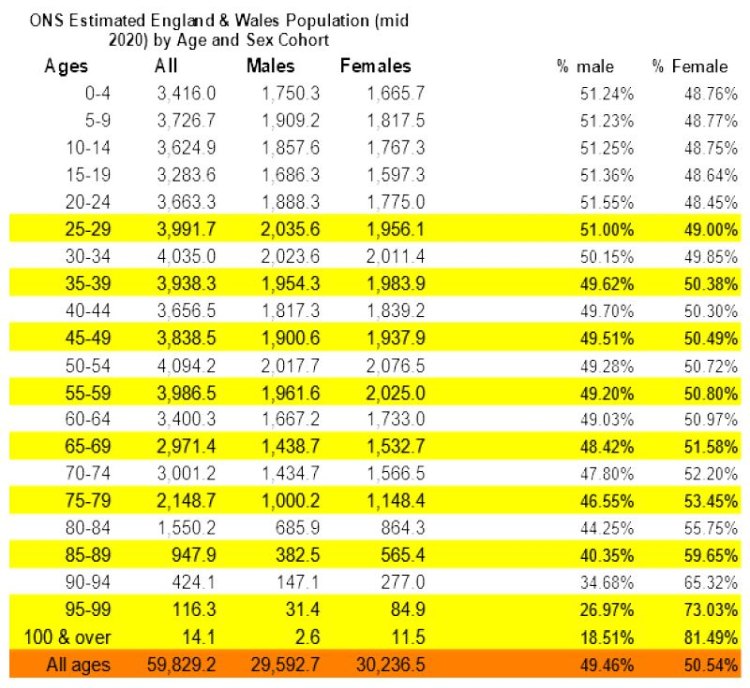
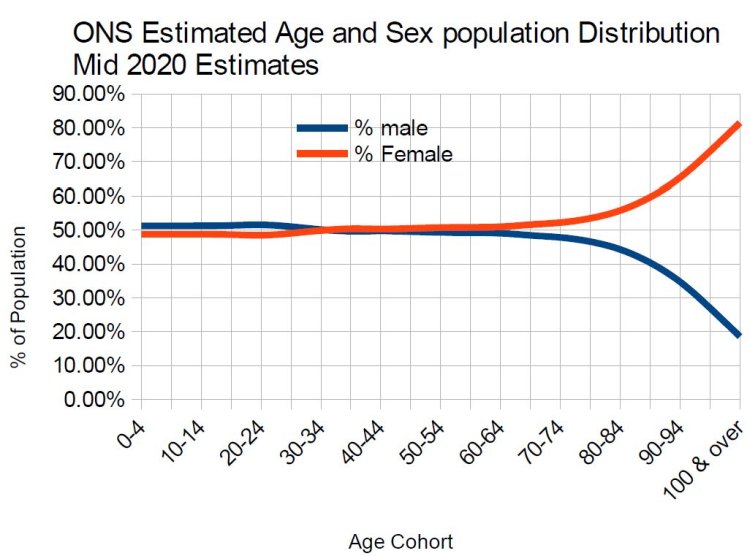
For the overall population of England & Wales, there is a slight sex imbalance insofar as there are projected to be approximately 643,800 more females than males (50.5% and 49.5% respectively). This sex bias is, however, clearly not constant throughout the age cohorts. In common with the rest of the world (see https://ourworldindata.org/sex-ratio-at-birth), at birth and right through to the mid-30’s year old cohort there is a majority of males in England & Wales. At age cohorts greater than the mid-30s there is an increasing majority of females such that by the oldest age cohort of 100 and over, there are respectively only 18.5% males and 81.5% of females. Different patterns of male and female net migration could of course be partly responsible for this increasing feminisation characteristic of the older cohorts.
However, as will be shown shortly, by far the most important factor is the much greater premature death rates suffered by males vis-a-vis that of females.
Note, the age cohorts differ slightly between the two individual ONS data sources. It was therefore necessary to split the 0-4 into two separate categories (<0 and 1-4) and to aggregate the oldest three categories (90-94, 95-99, and 100 and over) into one new category (90+) to render the two datasets comparable. These 20 revised age cohorts were used in all subsequent analyses.
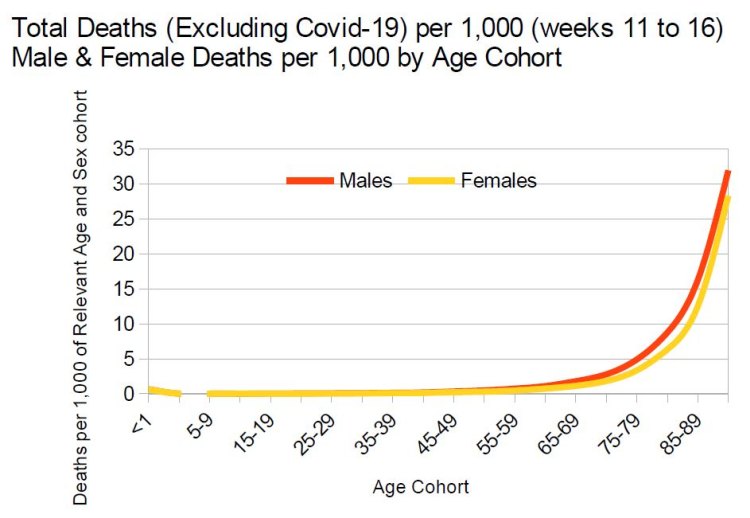
The table and chart below show the deaths from all other causes (i.e., excluding COVID-19) per 1,000 of the relevant age and sex cohort. From 15-19, males experience higher death rates than their respective females for all age cohorts. Deaths per 1,000 for males are below 1 in 1,000 up to the mid 60s age cohort and then rise quite steeply to 31.2 per 1,000 for the oldest 90+ cohort. The 1 in 1,000 deaths from all causes (excluding COVID-19) for females is not reached until approximately 70 years old and then rises steeply to approximately 28.3 per 1,000 for the 90+ age cohort.
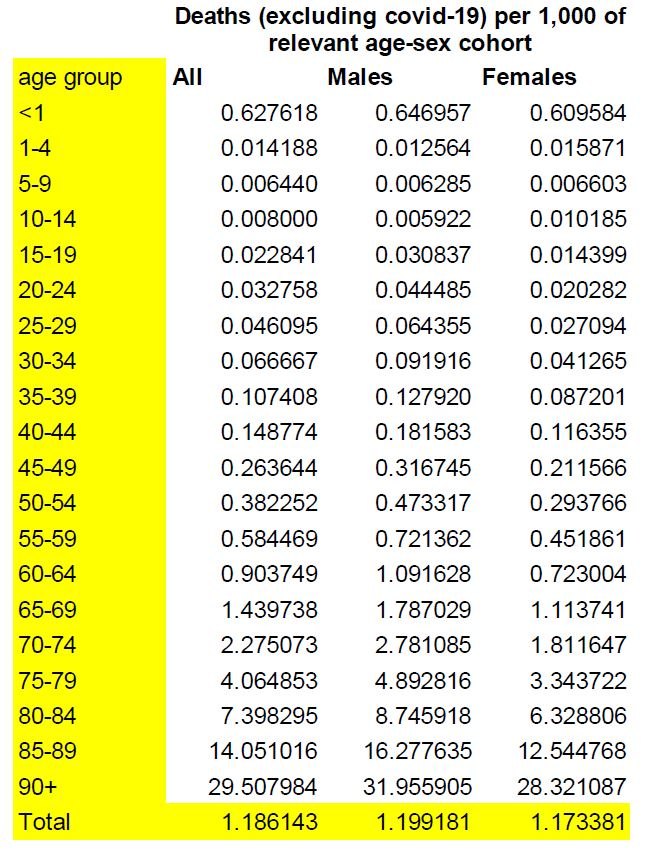
The chart below represents these patterns in graphical form. The red line represents male deaths from all other causes and the yellow line the female deaths.
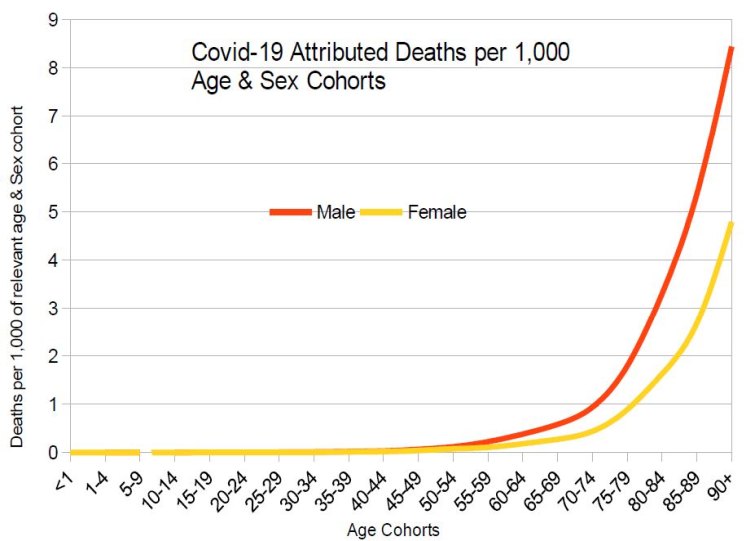
The alleged COVID-19 deaths per 1,000 by sex and age cohort are detailed in the table below.
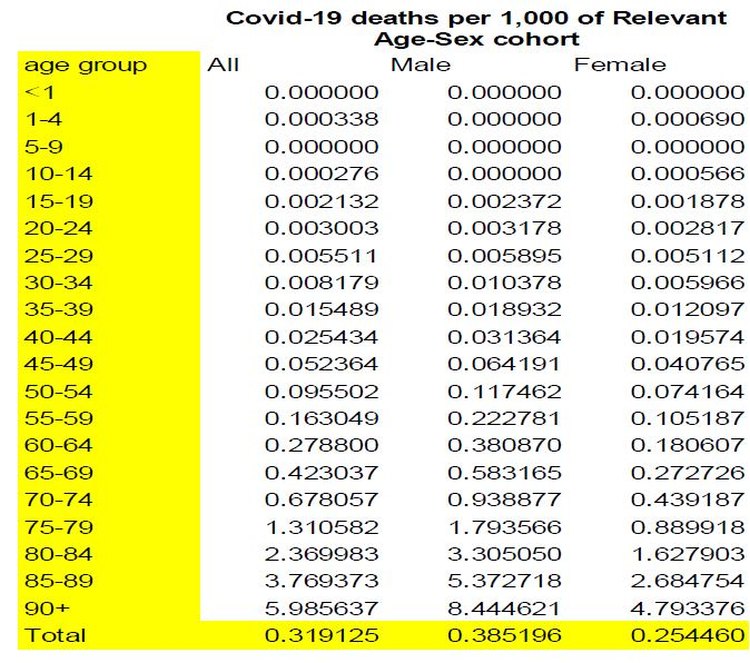
This presents a very similar pattern in terms of age and sex as for the all other deaths figures: males die off in greater numbers and at earlier ages than females and both sexes die off at increasing rates per 1,000 as we rise through the age cohorts.
Importantly, however, COVID-19 deaths per 1,000 are all much lower than for all other causes of deaths. For example, even for males in the oldest age cohort (90+), the COVID-19 deaths per 1,000 are only 8.4, whereas all other deaths for males in that age category are almost 32 per 1,000, which renders COVID-19 approximately 4 times less fatal than all other causes of death for males. Similarly, in regard to female deaths from COVID-19, from about the age of 60, males have around double the death rate from COVID-19 than that suffered by females. The 4.8 COVID-19 deaths per 1,000 suffered by the 90+ females is only around 1/6th of the death rate suffered by females in this age group from all other causes. Hence, COVID-19 deaths are generally of minor importance when compared to deaths from all other causes and that in regard to females, being fearful of COVID-19 is even less warranted than it ought to be in respect of males.
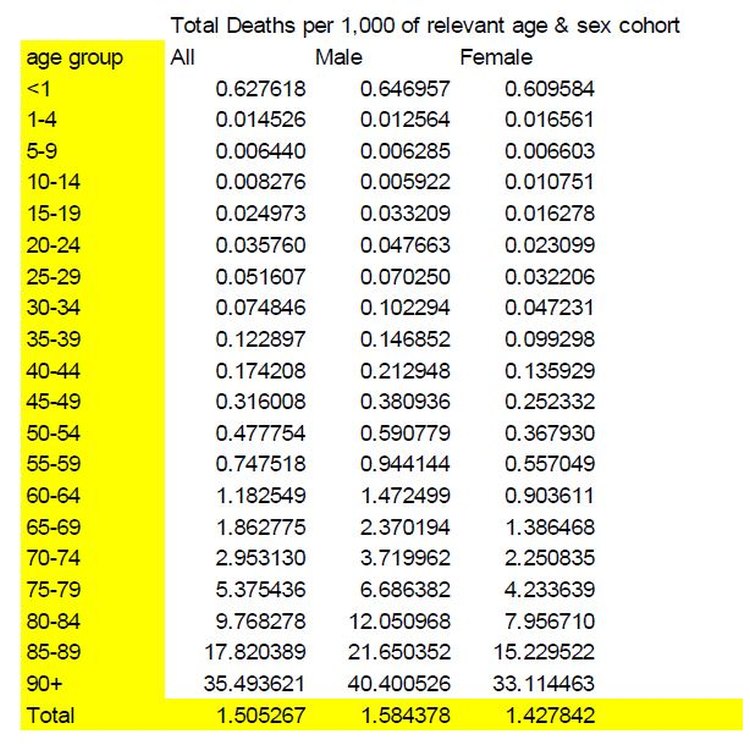
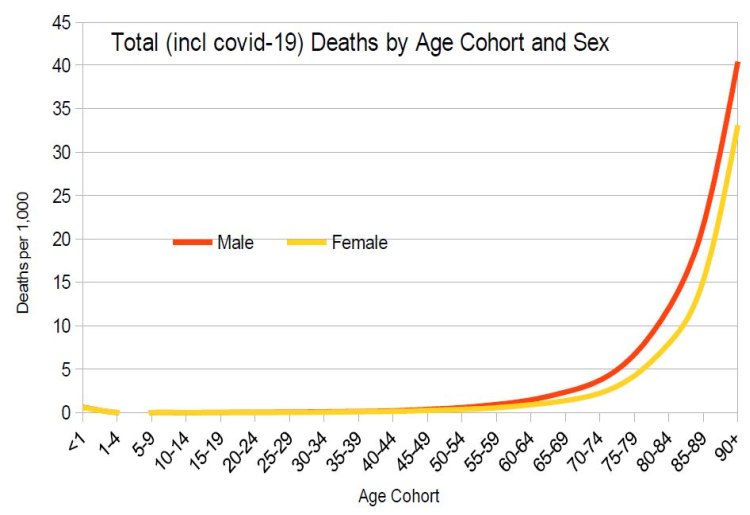
Finally, when Total Deaths From All Causes (including COVID-19 deaths) are tabulated by age and sex cohort, it can be seen that death remains a relatively rare occurrence for both sexes prior to the age of 60; approximately 1 in 1,000 for males at age 60 and slightly under 0.6 per 1,000 in respect of females of the same age. Relative death rates rise exponentially past this point for both sexes but at an even faster rate in regard to males, such that the highest age cohort has deaths per 1,000 of 40.4 and 33.1 for respectively males and females. This asymmetric sex pattern is evident from the graph below: compared to the total deaths (excluding COVID-19) functions, the sex specific total deaths (including COVID-19) functions become slightly further apart as age increases.
Incremental Impact of COVID-19 by Sex and Age Cohort
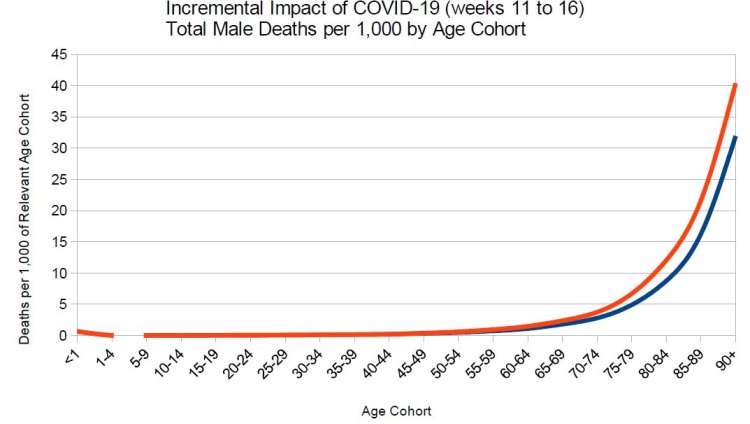
Below is the graph of Total Male Deaths Excluding Covid-19, the blue line, compared to Total Male Deaths Including COVID-19, the red line. Only after around the age of 70 is there any real difference (approximately 1 in a 1,000 difference) in death rates between the two functions. By the age of 90, the red line has an extra 8 deaths per 1,000 differential.
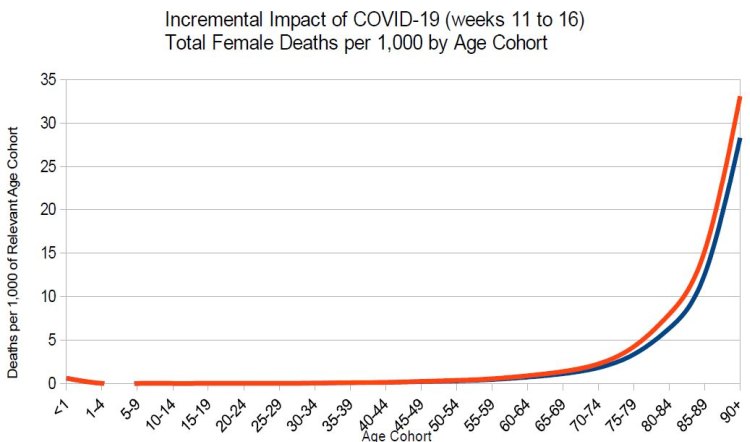
Below is the comparative female total deaths function (the red line) compared to the total deaths excluding Covid-19 function (the blue line). Here, it can be seen that the 2 lines are very close together. This reflects the fact that it is only after the age of 80 is there a 1 in a 1,000 increase in female death rates associated with COVID-19. This differential death rate only increases by 4.8 deaths per 1,000 in the 90+ age category.
In Conclusion
Covid-19 does not appear to be a significant new cause of death for the vast majority of the age range of the population of England & Wales. Indeed, deaths from all other causes swamp COVID-19 death rates even amongst the very oldest males. Female COVID-19 deaths are of even less significance than for males in that over 60% of female Covid-19 deaths occur in females 80 or more years old. As such, COVID-19 death rates appear to largely replicate (indeed, reinforce) normal or ‘natural’ death patterns, i.e., the elderly males and very elderly females are the only groups significantly impacted by COVID-19. In a less hysterical world, COVID-19 wouldn’t even register as a possible/probable cause of death to any relatively heathy individual below state pension age either in the immediate future or as they age further because in all likelihood today’s 65 year olds will develop immunity to this new disease and as a consequence COVID-19 will become considerably less deadly.
Note from Hector: Robert has sent through the spreadsheet he used in case anyone wants to check or extend it.
35 thoughts on “Robert Watson: A comparison of the relative magnitude of ‘COVID-19’ and ‘All other causes’ of deaths per 1,000 for age and sex cohorts”
Excellent piece of work, thank you.
This reinforces my impression that either this non-living entity, the virus is magical and mimics the health/illnesses of humans with supernatural abilities; or slightly more likely the vast majority of deaths are ‘with’ cv-19 and not ‘of’ cv-19.
As the Prof said, in a less hysterical world, and possibly one that is not in awe of computer models, we would now be getting on with our lives as normal.
@Robert Watson
Male/Female, Age – missing is Skin Colour
Royal College of Surgeons: BAME healthcare workers should be ‘removed from danger’ on frontline because they are ‘genetically more at risk of Covid’ despite it piling pressure on white NHS staff
Racisim is Now Good
UK Health Service Plans to Withdraw Ethnic Minorities from Coronavirus Frontline
COVID Update – Focus on Vitamin D
– drmalcolmkendrick.org/2020/04/28/covid-update-focus-on-vitamin-d/
Makes more sense than all the Left’s racist virus, UK deprivation & poverty etc rubbish. Maybe we should stop importing them as it increases their virus death rate
Ahem, I’ve been being racist and saying this for over a month and being mostly ignored eg:
One thing that I haven’t seen discussed, but which is important, is the matter of where people are catching CV-19. Those dying now would have picked up the virus during lockdown, so how are these mainly elderly people who are dying coming into contact with the virus when they are likely to be complying with the lockdown, social distancing rules?
I realise this is probably impossible to know, and that’s why it isn’t being discussed, but I’d be interested to hear theories and speculation.
The same question perhaps arises about prisons which might be regarded as the ultimate in lockdown. Yes I know, once the virus is inside it is likely to spread very quickly.
Thanks Prof. Watson, and good work.
I’m tempted by your very welcome analysis to say “So what’s new?” so, I will.
In my opinion, your piece is way overdue, (aware that statement’s a nonsense, as figures weren’t available) but Hooray! What we sceptics felt from the start and what should now be placed firmly under the noses of Ferguson, Hancock and Johnson, along with all the other prophets of doom. I should say that I’m 74, and male so I have what might be termed “a vested interest”, and I still say Hooray! and excellent work.
Thank you.
Who is the lady in the head picture ? – And why is she laughing at Robert’s article?
*whilst COVID-19 is most certainly a new cause of death, its victims are predominantly older men (75+) and very elderly women (80+)*
Excellent article. But surely corona viruses aren’t a new cause of death? I can’t remember where I read that CV-19 was “a virus with PR.” On the same theme Dr Wolfgang Wodarg in an excellent talk available on YouTube recorded pre-lockdown said ‘The emperor has no clothes’ – looks like the figures vindicate him.
It’s always been “good” when Europeans are the target. I live nearby the Marcus Garvey Centre (Garvey was a racial separatist) outside of which there’s a stone commemorating the death of Cynthia Jarrett who died of a heart attack as police were trying to arrest her son in 1985. PC Blakelock was hacked to death shortly after. The MP at the time said the police “got a bloody good hiding”. And that politician is a moderate compared to his successor. The racial antagonism is very real and bubbled over again in 2011 when the police shot a well known gangster. But this time police backed off while the “youth” looted and burned the High Road with impunity. In spite of the violence, which we’re supposed to imagine is never racially motivated, even when it manifestly is and even when it’s openly celebrated, Europeans don’t take race-hate or Afro-fascism, to use Stanley Crouch’s term, seriously. As we’re always reminded only a minority actually engage in violent crime of any kind. But whenever there’s conflict, when people have to choose sides, their loyalties are decided by race. Hence the absence of any memorial to PC Blakelock, the one man to suffer a violent death in the 1985 riots. There’s a plaque at Tottenham Police Station in memory of a policeman killed in 1909 but nothing to remember PC Blakelock. Racial loyalty is the rule for everyone except Europeans. As the great truth-teller of our time Rene Girard has put it in a broader context: ‘Not only is the revolt against ethnocentrism an invention of the West, it cannot be found outside the West.
Matt
Like almost all infections of this type once populated through care homes and hospitals they can cause mass infections and deaths of the most vulnerable ( flu like illness does this every year). Our local care home suffered after positive patient (infected in hospital) was returned to home and virus spread. These places are not isolated in the sense that people still work there and food/medicine etc still comes in and out. Staff circulate at home and in supermarkets etc so virus can still spread. This is all normal. The GOV have also re patriated thousands of citizens from all over the world who arrive home and are then locked in with family. Additionally we know that the virus is more widespread than early indications so the more we test the more we will find but most will be asymptomatic or have mild condition.
The time period, weeks 11 to 16 inclusive, was chosen due to week 11 (week ending March 13) being the week in which the first alleged COVID-19 death in England and Wales occurred, and week 16 (week ending April 17) being the week with the most recent figures to be published by the ONS (on the 28th April).
Most of this period was under lockdown, so strictly speaking it’s a comparison of the relative magnitude of ‘mitigated COVID-19’ and ‘all other causes’ of deaths.
I point this out for those who might wish to use this interesting piece as proof the lockdown was not needed*.
* I am against the lockdown.
I guess I had my suspicions that a lot of those dying might have picked up the virus in hospital. And of course the carehomes will be breeding grounds, especially once the hospitals have dumped Covid cases back into them.
I don’t actually think that supermarkets are particularly dangerous places to be. If they were, we would have seen a lot of disruption with staff becoming infected in large numbers. It took a while for the protective measures to be implemented and nowhere sees as many people pass through as a supermarket.
The left is clamouring to release prisoners at risk while insisting that the rest of us stay imprisoned at home to prevent risk.
It would be great if the hydroxychloroquine regime were deemed an acceptable option by U.K. medical authorities. “80 Patients and Staff Members Come Down with Coronavirus at Texas Nursing Home – Hydroxychloroquine Treatment Saves All But 1 Patient”, reports Gateway Pundit this week.
I have worked closely with computers since 1972 – hardware, software, methods, theory, etc.
And I find it astonishing that so many people pay superstititous reverence to computer models. After all, they are nothing more than drastic simplifaction of real systems, expressed purely in mathematical terms, and then revved up to computer speed.
As the old in-joke goes, “To err is human. But to really foul things up on an industrial scale, you need a computer”. Another way of putting it is, “Garbage in, garbage out”.
The great John Maynard Keynes warned, a century ago, that “To convert a model into a quantitative formula is to destroy its usefulness as an instrument of thought”.
Why is this? Well, a computer model is simply someone’s theory automated and made to run very, very fast. It can accept, process and take into account vast amounts of data – which people can’t – and that allows it to come to absurd conclusions that no reasonable human would consider for a single moment.
But just because it comes out of the computer, which still has an aura of godlike wisdom – like the oracle at Delphi – everyone assumes it has some special truth and reliability.
It doesn’t. If Dr Ferguson’s ideas are wrong, then his model will be wrong. And his ideas are wrong.
One hundred and fifty eight years ago, the inventor of the mechanical computer summed it up in a nutshell.
“On two occasions I have been asked, ‘Pray, Mr. Babbage, if you put into the machine wrong figures, will the right answers come out?’ I am not able rightly to apprehend the kind of confusion of ideas that could provoke such a question”.
– Charles Babbage, Passages from the Life of a Philosopher, 1862 (first mention of “GIGO”)
It would be great if the hydroxychloroquine regime were deemed an acceptable option by U.K. medical authorities. “80 Patients and Staff Members Come Down with Coronavirus at Texas Nursing Home – Hydroxychloroquine Treatment Saves All But 1 Patient”, reports Gateway Pundit this week.
I think it is honest and quite “unracist” to say that black people evolved in Africa and therefore their skin is suitable to keep them healthy under a hot tropical or semitropical sun. After all, if the anthropologists are right, we all evolved in Africa.
When people migrated out of Africa to colder regions with less sunshine, their skin gradually adapted to become paler and thus to generate more Vitamin D from what ultraviolet light was available.
Today, if a person whose ancestors lived in Africa until no more than a few hundred years ago comes to live in a cold climate, that person will risk having seriously inadequate Vitamin D. (As, indeed, do a lot of white people too). So they would do well to supplement the vitamin.
It is a great shame that the NHS has never understood that need, nor taken any steps to give its BAME employees (at least, not to mention patients) the necessary supplements.
That’s not “racist”. It’s science (and common sense).
The slight excess of males at birth is, I understand, normal mammalian biology. Males take more risk, die earlier, so long as they don’t Darwinate mission accomplished; females need to be more cautious and survive long enough to nurture viable offspring.
But once beyond normal reproductive age we are all surplus to Nature’s requirements, maybe there will be herd immunity and life expectancy at the old normal, at the moment CV-19 is culling the herd.
One has to hope analysis very similar to this is being force fed to government ministers. This lockdown has to now end. Even my eminently sensible 20 year olds who moved back home for the duration are both now losing the plot, as their mates. If the lockdown doesn’t end with the evidence suggesting it should, it will end up being broken by mass disobedience
Excellent observation Matt. Makes standing queuing out in the rain look a bit pointless!
Uptick.
Yes! And that’s why all this waiting for a vaccine is nonsense.
Nick A: “If the lockdown doesn’t end with the evidence suggesting it should, it will end up being broken by mass disobedience
Look at the Lockdowns as part of a Manichean struggle between the ruling Political Class and us peons. If the Political Class wins and keeps its boot firmly on our mostly willing necks, then it is goodnight Western civilization. If we peons win through a process of mass disobedience, the social compact between us and the Political Class will have been irretrievably broken. Once mass disobedience shows that the Law is toothless, we all become Hillary Clinton — above the Law. Once again, goodnight Western civilization.
To return to my underlying fear, if the rulers of China had been looking for a way to castrate their enemies in the West, they could not have done better than triggering our Political Class’s over-reaction to Covid-19.
I have to wonder if doctors would agree to treat me with HCQ if I were to contract the virus. I would certainly request it but would they agree? Would I be able to force the matter?
I’m not sure how it works.
The death rate in French hospitals has dropped substantially since Macron met Raoult and put him in charge of HCQ treatment in hospitals.
Speculation is rife that Boris was given HCQ, which matches up with the 6 day schedule.
Rumour has it that some of the medical establishment were prepared for the PM to croak rather than admit a cheap generic Trump pill could work.
Seems the French have detected Covid in samples taken from patients that had undiagnosed respiratory problems in December, which would surely skew the figures used for the virus and the timing for lockdowns. Does tie in with anecdotal evidence of a flu type bug going around at the time. A friend worked on local equivalent of ask the NHS 111 advice number and said they had a big uptick in flu cases reported late December early Jan
I decided to change that picture for something more low-key.
I can remember working on a bit of software that managed to generate the right result for the wrong reason in some circumstances! We should always remember that GIGO doesn’t just apply to input data, it applies to the code as well.
Yes Nick, you couldn’t make it up – but they did.
Without getting too political – the left’s world-view is stuffed with contradictions so glaring how can they survive, such as their support for any gender position, while at same time supporting the one world-view that opposes that position.
The events following the release of Michael Moore’s “Planet of the Humans”, can be summarised as capitalism is the world’s biggest problem, unless of course you are one of “OUR” capitalists. The cronies called out in the film (a must see on YouTube if you have not) would have been vilified had they been of “the right”. Koch brothers, mind you, appearing in both guises in the film.
OH NO! Nick. We can’t use that – Orange Man Bad mentioned it. Sorry Sarc off/
Trump Derangement Syndrome (TDS) is killing people – Comment by MIchel Jenkins in the USA
“Am I the only one who has noticed that, as of May 1 statistics on Worldometer.com, Michigan, whose governor is ruling like a Central American dictator and who threatened doctors with jail if they prescribed HydroChloroquine to COVID patients, has the highest death rate (9.1% of reported cases) of any state?
At the other extreme, South Dakota’s governor decided early on to keep the state open for business, while suggesting sensible precautions, and the governor announced that her state would be a testing ground to see if HydroChloroquine works. The death rate in South Dakota is the lowest of any state, at 0.83%.
If “following the science” meant following the data, instead of following politically biased scientists over a cliff, those results should be the opposite of what we’ve seen.”
My son and a friend were both ill in early January. Son had a dry cough and fluey symptoms. Friend had a raging temperature and was diagnosed with pneuonia and treated with antibiotics..
My niece works in a big Tesco warehouse near London, and she said there was a very nasty flu going around Dec Jan, many off work. She had it and was off for weeks.
Robert: very interesting analysis, my only nitpick would be that comparing Covid deaths to all deaths is slightly misleading. A better feel for the severity of the disease would be a comparison to any one other cause of death (or a previous year’s flu deaths)
John
Science *is* racist, according to the progressives. We need more “inclusive” mathematics, believes Prof Sara Hottinger of Keene State College, while Professor John Caputo of Syracuse Uni goes further, suggesting that the exercise of reason itself is just a “white male Euro-Christian construction.”
Comments are closed.